Cardiology Closed Claims Study
The Doctors Company conducted a review of diagnostic cardiology claims that closed between 2014 and 2019. This study was based on claims and lawsuits filed against almost 500 cardiologists insured by The Doctors Company. There were 210 cardiology claims.
Fear of COVID-19 Creates Its Own Risks for Cardiologists
“In polling cardiologists across the country, I’ve learned that one area in which almost all have seen or heard cases about are those who were to undergo transcatheter aortic valve replacement (TAVR) who did not undergo the procedure, and died,” said John P. Erwin, III, MD, FACC, a cardiologist at NorthShore Medical Group.
Dr. Erwin’s comments illuminate a common theme for cardiologists during COVID-19: the risks of delayed care. While avoiding infection risks, patients may experience increased risks from existing or new cardiovascular conditions—and cardiologists may thereafter find themselves at increased risk for medical malpractice lawsuits.
Technologies for maintaining continuity of care can contribute to the problem: While telehealth in the form of remote monitoring has been well adopted by cardiologists, telemedicine visits can present serious challenges to diagnosis. Dr. Erwin says, “Cardiologists are usually astute diagnosticians, and part of that relies upon being able to lay eyes and hands and stethoscopes on the patient to determine risk/acuity level.”
While telemedicine visits have helped keep vulnerable patients home when practical, when cardiologists alert patients that they truly need to come to the clinic setting for evaluation, some will refuse to do so out of infection fears—sometimes with dire consequences. A recent JAMA Cardiology article noted that while some cardiologists have been supporting colleagues in critical care, many acute care settings “remain eerily quiet. Recent data from 9 high-volume centers across the US suggest a nearly 40% drop in catheterization laboratory activation for ST-elevation myocardial infarction care during this crisis. Apparent fear of COVID-19 is having the direct outcome of decreasing the use of life-saving evidence-based treatments.”
This decrease in patients accessing life-saving treatments may later yield an increase in claims of medical malpractice: Patients may suffer a catastrophic event or simply seek treatment when their disease is at a later, more advanced stage, with treatment options more limited and outcome prospects less favorable.
COVID-19 delivers a freight of risks that cardiologists cannot control—adding motivation to mitigate the risks they can control, or at least influence. Through reading this careful analysis of recent cardiology malpractice claims, cardiologists can elevate their awareness of cognitive and system factors contributing to adverse events.
Attending to these factors can help cardiologists protect patients and mitigate their risk of claims.
Regardless of the outcome, all diagnostic cardiology claims against our members that closed within this time frame were included in this analysis. This approach helps us better understand what motivates patients to pursue claims and helps us gain a broader overview of the system failures and processes that result in patient harm.
This study, reinforced by expert insights and relevant case examples, focused on the following areas:
- Most common patient injuries.
- Injury severity.
- Most common types of diagnostic cardiology malpractice claims.
- Factors contributing to patient injury.
- Strategies for mitigating risk.
Our approach to studying diagnostic cardiology malpractice claims began by studying patients’ injuries to understand the full scope of harm. Physician experts for both the plaintiffs/patients and the defendants/physicians reviewed claims and conducted medical record reviews. Our clinical analysts drew from these sources to gain an accurate and unbiased understanding of actual patient injuries.
We then looked at the types of cases to capture the key clinical areas or case types. Identifying these clinical drivers helped us to focus on the causes of patient harm and the things that prompted patients or their families to file claims and suits.
We identified factors that led to patients’ injuries, and physician reviewers evaluated each claim to determine whether the standard of care was met. Contributing factor categories included clinical judgment, technical skill, patient behaviors, communication, clinical systems, clinical environments, and documentation.
Our team studies all aspects of the claim and identifies risk mitigation strategies that physicians can use to decrease the risk of injury, thereby improving the quality of care.
Patient Injuries
Cardiology patients suffered a variety of injuries. The 10 most common injuries that prompted claims or suits included:
Patients may suffer more than one harm, so the total is greater than 100 percent.
Injury Severity
Injury severity has not changed significantly in the last 12 years. A comparison of the 2008–2013 study with the 2014–2019 study shows only 1 percent difference in the number of cardiology patients who experienced a high-severity injury, the largest category of injuries.
Cardiology Patient Injury Severity 2014–2019
Cardiology Patient Injury Severity 2008–2013
Indemnity and Expense
Thirty-one percent of cardiology claims resulted in a payment to the patient or their family.
$375,313
Mean indemnity paid
$138,526
Mean expense paid
$225,000
Mean indemnity paid
$106,614
Mean expense paid
Rate of Claims Per 100 Full-Time Equivalents
The rate of claims for cardiologists has declined most years from 2005 until 2018. The high was 11.4 percent in 2008 and lows were recorded at 6.0 percent in 2014 and 2015.
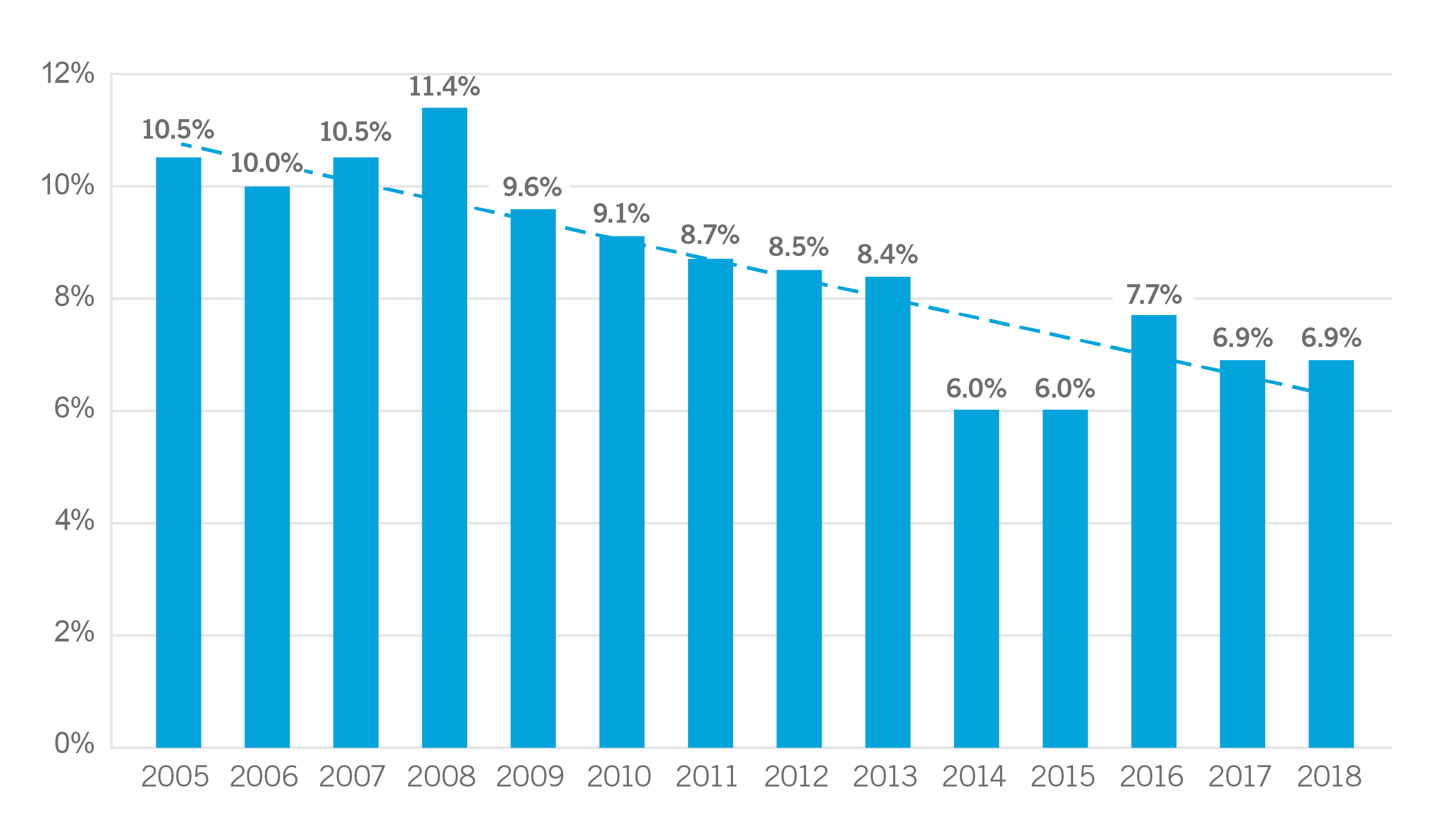
Overall, the number of claims filed against cardiologists has decreased over the last 14 years. However, it could be argued that the rate of claims in the last five years is starting to increase. Either way, it is important to explore ways of reducing the number of patient injuries.
Regardless of the trendline, claims and suits that have been filed continue to have a high percentage (67 percent) of high-severity injuries. A focus on these cases yield insights that help reduce the frequency and severity of patient injuries.
Site or Type of Facility
Most cardiology claims arose from care provided in the hospital setting (59 percent). Physician offices were the second most common site (34 percent). The other 7 percent were spread between psychiatric hospitals (1 percent), ambulatory surgery centers (1 percent), skilled nursing centers (1 percent), and unknown (4 percent).
Within hospitals, the most common locations for care that resulted in claims were patient’s room (29 percent), cardiac catheterization lab (13 percent), special procedures (6 percent), intensive care units (6 percent), operating rooms (5 percent) and emergency departments (3 percent).
Sex of Patients
The frequency at which males and females are represented in cardiology claims has remained consistent since our last study in 2014.
Cardiology Claims by Sex 2014–2019
Cardiology Claims by Sex 2008–2013
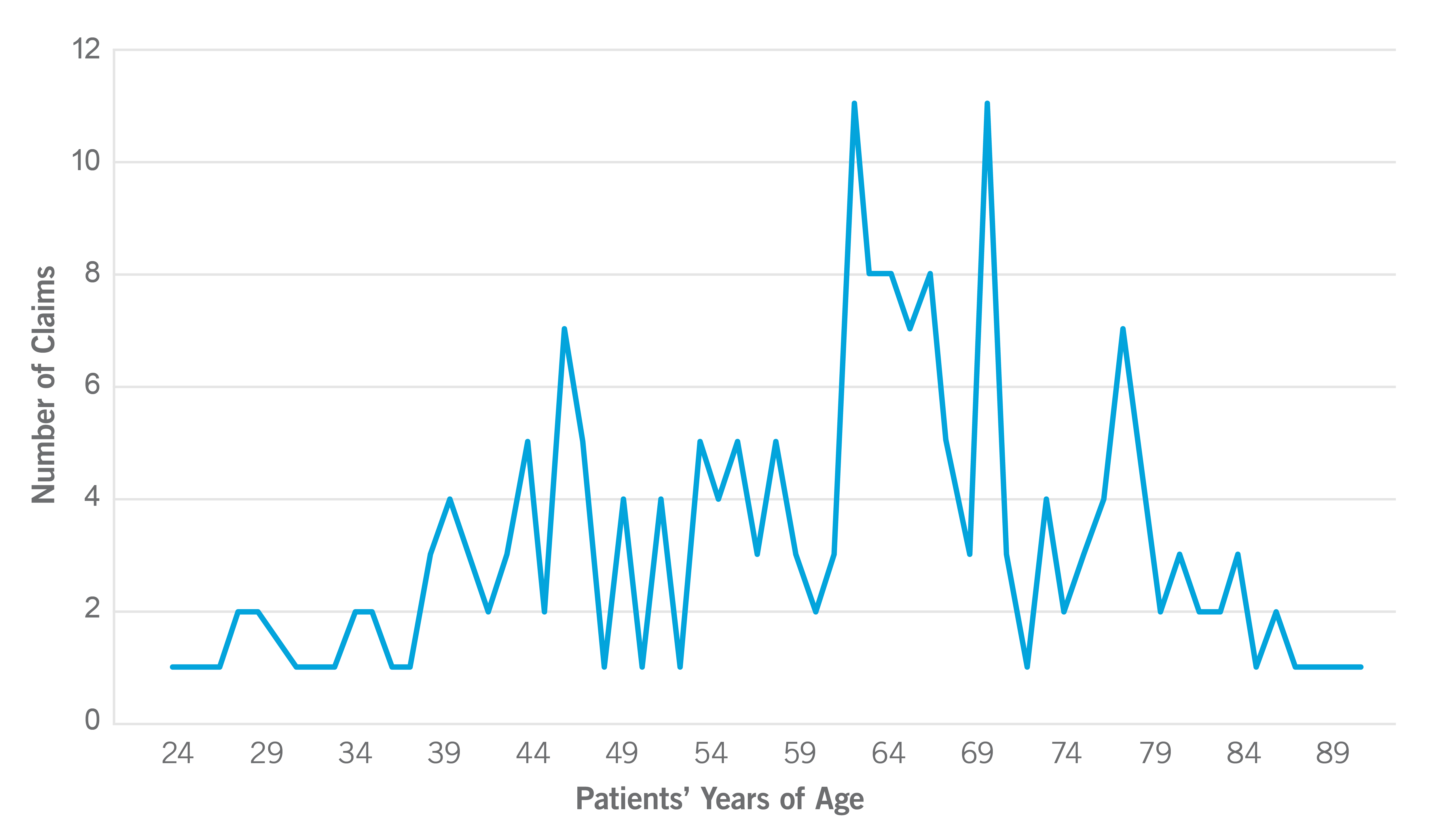
Ages of Cardiology Patients
The peak age range for cardiology patients at the time the alleged injuries occurred was 63 to 71. Other, smaller peaks were seen in the mid-40s and again in the late 70s.
Types of Claims
There were five primary types of cardiology claims:
These case types make up 74 percent of cardiology claims.
Diagnosis-Related Claims
Diagnosis-related claims made up 33 percent of cardiology claims. The 10 most frequent final diagnoses associated with diagnosis-related cardiology claims were aortic aneurysm (15 percent), acute myocardial infarction or cardiac arrest (13 percent), atherosclerosis of native coronary (11 percent), acute and subacute endocarditis (8 percent), pulmonary embolism (4 percent), cerebral artery thrombosis or occlusion (4 percent), malignant neoplasm of bronchus or lung (4 percent), cardiac dysrhythmia (3 percent), congestive heart failure (3 percent), and central nervous system complications (3 percent).
On average, three to four contributing factors are coded on each claim. In this study, the factors that contributed to diagnosis-related claims included inadequate patient assessments (76 percent of diagnosis-related claims), failures in communications among providers (26 percent), patient factors (21 percent), lack of communication between patients/families and providers (17 percent), errors in selection and management of therapy (16 percent), failure or delay in obtaining a consult or referral (16 percent), and insufficient or lack of documentation (14 percent).
The most common factor, inadequate patient assessments, is consistent with the most common case type, diagnosis related (failure, delay, incorrect). Assessments were found to include delays in ordering diagnostic tests that were identified by physician reviewers. Another factor was failure to appreciate and reconcile relevant signs, symptoms, and test results. Misinterpretation of diagnostic studies was another deficiency in these assessments.
Failures in communication occurred among providers. Some were due to failing to review all relevant information in patients’ records. On other occasions important information was lost in transitions of care and/or handoff communication.
Patients’ behaviors were a factor in one out of five cardiology cases. Patients either refused to have tests performed or were not adherent to treatment medication plans. It could not be determined from this study whether patients failed to understand information provided by their cardiologist or decided not follow advice for reasons such as fear or lack of resources to pay for the care.
Factors that contributed to patient harm:
- Inadequate patient assessments (76 percent)
- Failure or delay ordering diagnostic tests
- Failure to appreciate and reconcile relevant signs, symptoms, or test results
- Misinterpretation of diagnostic studies
- Failure to establish a differential diagnosis
- Narrow diagnostic focus with an atypical presentation
- Failures in communication among providers (26 percent)
- Regarding the patient’s condition
- Failure to read medical record
- Information lost during transitions of care and/or handoff communication
- Patient factors (21 percent)
- Patient not adherent to follow-up appointments
- Patient not adherent to medication or treatment plan
- Lack of communication between patients/families and providers (17 percent)
- Regarding follow-up instructions
- Regarding patient’s expectations
- Errors in selection and management of therapy (16 percent)
- Invasive procedures
- Medical treatments
- Failure to order medications
- Failure or delay in obtaining a consult or referral (16 percent)
- Insufficient or lack of documentation (14 percent)
- Regarding clinical findings
- Regarding clinical rationale
- Regarding follow-up efforts
The patient was a 59-year-old female with a history of hypertension, smoking, COPD, and abdominal aortic aneurysm. She presented to her primary care physician’s office with neck, chest, and abdominal pain. She was dizzy and weak. The patient was evaluated by a nurse practitioner (NP).
A chest x-ray showed vascular congestion with interstitial edema. The NP diagnosed cervicalgia. No cardiac workup was done.
Three days later, the patient presented to the emergency department complaining of sharp chest pain radiating to her shoulders. The pain had started two days prior.
The emergency physician diagnosed unstable angina after reviewing a troponin level of 0.48 and an EKG with a non-STEMI interpretation. He admitted the patient to ICU with a cardiology consult.
A chest CT showed no thoracic aneurysm. A hospitalist ordered Lovenox. The cardiologist ordered serial cardiac enzymes. The patient continued to experience significant chest pain even with administrations of nitroglycerin and Dilaudid.
An EKG showed anterior Q waves. The cardiologist opined that the patient had experienced a myocardial infarction that was two days old. He planned a cardiac catheterization the next day.
Due to increasing troponin levels and an echocardiogram that showed significant left ventricular dysfunction, the cardiologist took the patient for a cardiac catheterization later the day of admission.
That study showed 100 percent occlusion with thrombus of the left anterior descending artery. He performed angioplasty and placed a stent. The patient’s ejection fraction (EF) remained between 30 and 35 percent.
Over the next few days, the patient became hypotensive with respiratory distress and pulmonary edema. She complained of shortness of breath before experiencing cardiac arrest. Resuscitation attempts were unsuccessful.
When a claim was filed, plaintiff experts opined that the patient’s acute coronary syndrome was not timely diagnosed or treated. The delay led to the patient’s decline and death.
Defense experts provided mixed reviews. Some testified that Q waves on the EKG indicated older infarctions. The nurse practitioner should have conducted a cardiac workup or sent the patient to the emergency room. The cardiologist should have taken the patient immediately to the cardiac catheterization lab. They believed that the delay caused increased muscle death and resulted in cardiogenic shock, congestive heart failure, and respiratory distress.
Even though most damage was done before the patient arrived at the hospital, further damage could have been prevented with rapid diagnosis and treatment. The NP, primary care practice, emergency physicians, and cardiologist all agreed to settle the case.
The patient was a 47-year-old male who had a history of Mallory-Weiss tear and type one thoracic ascending and descending aortic dissection five years earlier. The ascending dissection was repaired, but the residual descending aortic dissection was left unrepaired, due to potential surgical complications that could include paraplegia. The patient was followed by a cardiologist who monitored his blood pressure and conducted annual echocardiograms.
The patient presented to his primary care physician with complaints of back pain that had started the prior week. The patient reported no trauma or nausea. He also reported that the pain resolved at one point but then returned below his shoulder blade. Later the pain wrapped around his abdomen and up into his neck and throat and lasted for an hour. Pain medication helped reduce the pain.
Upon examination, the patient’s back was not tender upon palpation. He experienced no pain when bending or twisting at the waist. His lungs were clear. He appeared anxious.
The primary care provider thought that the patient’s pain could be a sign of shingles. However, the physician ordered a chest x-ray that was performed later that day.
At home the next day, the patient retrieved an ice pack from the refrigerator for increased back pain. A short time later, the patient cried out and collapsed. He was transported to the hospital emergency room where he was pronounced dead. The previous day’s x-ray was read after the patient expired.
The chest x-ray interpretation noted a massive enlargement of descending thoracic aorta. The patient died of a ruptured dissecting aortic aneurysm.
A claim was filed against the primary care provider, cardiologist, and cardiac surgeon. Considering the patient’s history, experts testified that the primary care provider should have included dissecting aortic aneurysm on the differential and sent the patient to the emergency department immediately. They said that the patient’s symptoms were classic for dissecting aortic aneurysm.
The cardiologist and cardiac surgeon were also criticized. The cardiac surgeon should have communicated a plan for regular follow-up to the cardiologist and primary care provider. The cardiologist should have consulted with the cardiac surgeon on periodic monitoring. The annual echocardiograms performed by the cardiologist were not the appropriate tests for tracking the patient’s condition. He should have ordered annual CT scans to monitor the aorta.
Experts agreed that with a good plan for monitoring and early diagnosis of the new dissection, the patient had had a reasonable chance of survival. All parties agreed to settle the case.
Risk Management Strategies to Prevent Diagnostic Errors
- Take a detailed medical history and conduct a thorough patient assessment—patient complaints are an essential source of information to assist cardiologists in making correct diagnoses.
- Consider and document differential diagnoses for all new problems or recurring, unresolved signs and symptoms. Timely diagnosis and treatment often depend on how quickly diagnostic studies are performed, interpreted, and acted on.
- Beware of breakdowns in communication, which have been associated with diagnostic error. Communication occurs during various parts of the diagnostic process, such as the initial patient assessment; tests, results, and processing; follow-up, and coordination. In today’s hurried healthcare environment, it is essential that cardiologists not only provide the information to the patient, but that the patient provides some response to that information that confirms understanding. Consider adopting a quick, structured approach to confirming understanding such as Ask Me 3.
- Respond quickly to the results of tests that have been ordered. This is key to timely diagnosis. Track studies and follow up on critical test results. If results are delayed, notification should come from the testing department (laboratory or radiology, for example). If test results are not received when expected, follow up to determine the cause of the delay. This step may reduce unnecessary delays in diagnosis and treatment.
- Be alert for ancillary findings of imaging studies. Lung nodules or other findings indicative of possible malignancy need to be addressed. Be sure to alert primary care providers and patients of these findings to make sure that follow-up diagnostic studies are performed and care is provided.
- Assess for depression. Studies show as many as 30 percent of post heart attack patients may experience depression
Improper Management of Treatment Claims
Improper management of treatment was the second most frequent case type. The final diagnoses most frequently associated with improper management of treatment included:
Fourteen other diagnoses made up 2 percent or less of cases each.
Improper management of treatment was found to be due to inadequate assessments (40 percent of these cases). Physicians failed to appreciate and reconcile relevant signs, symptoms, and test results when patients had unresolved symptoms. In some cases, it was determined that physicians failed to order or delayed ordering diagnostic tests or misinterpreted the diagnostic studies when they received them.
There were also alleged errors in selection and management of therapy. They included selection of medical treatment, selection of medications, and failure to order medications.
Inadequate communication between patient or family and provider was the third most common factor leading to patient injury. Patients needed more information about treatment options, patient education regarding the risks of medications, and discussion regarding their expectations about the outcomes of care.
A 67-year-old male presented with chest pain, shortness of breath, and troponin level of 3.27. The impression was non-STMI. A chest x-ray showed right lower lobe infiltrate.
The patient was admitted to the hospital. His oxygen level was 92 percent on four liters of oxygen. During the night, the patient complained of chest pain. His nurse administered morphine but did not notify the cardiologist.
The following morning the patient indicated that he did not have chest pain. His troponin was 0.47. Late morning, the patient began to complain of stabbing pain in his chest that was radiating to his left shoulder. He had diaphoresis. A nurse administered 5 mg of morphine but did not contact the cardiologist.
That afternoon the cardiologist evaluated the patient and found him to be asymptomatic. Also, cardiac enzyme values were decreasing.
During the night, the patient experienced atrial fibrillation but had a normal sinus rhythm the following morning. That day an echocardiogram showed an EF of 50 percent with moderate mitral valve regurgitation and pulmonary hypertension.
The patient appeared to be stable, so a cardiac catheterization was planned for the following morning. However, at 10:00 PM, the patient began to complain of severe chest pain. His nurse administered 5 mg morphine but did not call the cardiologist. The pain improved over the next 30 minutes.
At 3:30 AM, the chest pain returned. The patient was pale and diaphoretic with nausea. Chest pain improved but the patient experienced severe chest pressure and shortness of breath. His oxygen level dropped to 81 percent and his blood pressure dropped to 87/49 and continued to decrease. A respiratory therapist was called at 6:10 AM and a code was called five minutes later.
The cardiologist was notified and suspected that the patient experienced a pulmonary embolism. Before a CT scan could be performed the patient expired.
An autopsy showed cardiomegaly, left ventricular hypertrophy, and severe coronary artery disease. No clots were found in the arteries.
When the claim was filed, the plaintiffs took the position that the cardiologist should have ordered Plavix due to non-ST wave elevation myocardial infarction. They opined that the patient did not exhibit symptoms of a pulmonary embolism.
Defense experts were supportive of the treatment plan, stating that the patient did not need Plavix because no clots were found. Also, giving an anticoagulant would have postponed any surgical interventions. They agreed with the medical treatment approach for non-STMI while the patient was stable. The next step would have been cardiac catheterization as the patient’s condition became worse. They believed it was acceptable to wait to perform the cardiac catheterization.
Defense experts went on to state that they believed that the patient died of an arrhythmia. Their only criticisms were of the nurses who failed to notify the cardiologist of changes in the patient’s condition. However, they believed that the treatment would not have been different. The case against the cardiologist was resolved in favor of the defendant.
A 56-year-old patient presented with history of hypertension, type II diabetes, and occasional atypical chest pain. His primary care provider referred him to a cardiologist for a stress test, which showed reversible ischemia.
The cardiologist told the patient that he probably had significant coronary artery disease and recommended coronary angiography. The patient refused, but the cardiologist failed to document the patient’s response to this recommendation. The cardiologist ordered a calcium study, intending to use the expected elevated result to convince the patient to have the coronary angiography performed.
Before the cardiologist was able to discuss the elevated calcium result, the patient was involved in a car accident. During emergency treatment, it was discovered that the patient had an abnormal EKG, prompting further studies and stenting of one coronary artery. It was 99 percent blocked. He was placed on anticoagulants. The patient recovered from the procedure and his injuries from the car accident.
Following his recovery, the patient was encouraged to follow up on additional cardiac studies. The patient chose not to seek additional testing and treatment.
Five months later, the patient experienced a cardiac arrest. The patient survived but had weakness in both lower extremities. This was thought to be due to in part to his diabetes.
The patient filed a claim alleging improper management of his treatment. Experts were mixed in their reviews of this case. Some thought it a breach of the standard of care to order a calcium study rather than an angiogram. Other experts said that the patient needed an angiogram as soon as possible and that the cardiologist should have ordered aspirin and a statin.
Failing to document the patient’s refusal to have coronary artery angiography increased the difficulty of defending this case. The case settled against the cardiologist.
Risk Management Strategies to Prevent Improper Management of Treatment
- Consider all symptoms and test results when making treatment recommendations—and communicate how these symptoms and test results yield various choices available to the patient, so that they can make informed decisions. Document all informed consent discussions.
- Be accessible and responsive to nurses. Build rapport. When nurses call to report changes in patients’ status, respond to their concerns. Ask nurses if they think that you should evaluate the patient. If they say no, ask, “Are you sure?” This communicates a message of trust in nursing judgment and will encourage future calls when nurses have concerns about the patients in their charge.
- Treat handoffs and referrals as essential processes in good care. Foster healthy relationships with other clinicians. Provide them with the information that they need to effectively receive handoffs or to provide consultations.
- Communicate concerns and fears to nurses about specific patients. Prepare them to receive pending test results and provide guidance on how to respond.
- Review all documentation to ensure that you are aware of all consultation reports, consultant orders, and any changes to the patient’s condition documented by nursing.
- Encourage cardiac rehabilitation. Over the years, research has shown that patients who participate in cardiac rehab programs have better outcomes compared to those who do not participate.
Improper Medication Management Claims
The third most common case type was improper medication management. These cases arose from selection of medications, nonadherence by patients to medication and other treatment plans, and inadequate education regarding the risks of medications.
In most of these cases, the care and treatment were found to meet the standard of care.
A 69-year-old female with a history of mitral valve replacement, COPD, smoking, congestive heart failure, and chronic A-fib was on anticoagulants (Coumadin) for several years. At her routine checkup, her INR was 2.8 and PT was 18.8.
Due to the elevated results, the patient was advised to hold the Coumadin that day and take 5 mg per day for the next six days and 7.5 mg on the eighth day. She was asked to return to the office for testing on the ninth day.
On the eighth day, the patient received an order for an antibiotic from her pulmonologist for a urinary tract infection. When the patient presented for testing on the ninth day, her INR was 7.8 and her PT was 32.6. Repeat tests showed INR at 6.8 and PT at 66.7.
Noting that an antibiotic can affect coagulation studies, the cardiologist told the patient to not take her Coumadin for the next two days. He asked her to return the third day for repeat testing.
The day before her next tests, the patient was transported to the emergency department complaining of right-side weakness. The examination showed that the patient was alert, her cranial nerves were intact, and her oxygen level was 94 percent. An EKG showed atrial fibrillation with right bundle branch block. The chest x-ray showed cardiomegaly and early congestive heart failure. The PT was 57.4 and INR equaled 6.3. The patient began to complain of headache, and a CT showed acute subdural hematoma.
The patient was treated with vitamin K and factor VII and transferred to a higher-level hospital. She was taken to surgery for evacuation of the subdural hematoma. Postoperatively, the patient was unresponsive, and she expired a short time later.
The patient’s family filed a claim alleging improper management of Coumadin and inadequate monitoring. Defense experts were supportive of the care provided, stating that this patient had a complex history and that with long-term use of Coumadin, INRs can wax and wane even with proper control. The standard of care did require cessation of Coumadin and then testing, as was done in this case. This was an unusual complication that occurred even with good management. The case was dismissed.
Risk Management Strategies to Prevent Improper Medication Management
- Provide education on medications prescribed for the patient, including why the medication is needed, its risks, and its side-effects. Allow time for questions from the patient on these medications. Providing written materials on medications is beneficial.
- Document patient nonadherence or refusal to follow treatment plans. Use quotes from patient and family members. This documentation is essential in situations where cardiologists need to defend the care that was provided.
- Take time to build rapport with your patient. Increased levels of trust may result in a higher level of patient adherence to physician instructions and treatment plans.
- Request that patients bring all medication bottles to each clinic visit as part of the medication reconciliation process.
Improper Performance of Treatment or Procedure Claims
One case involved improper placement of a pacemaker, resulting in clavicle pain and the need for repositioning, as well as the use of a guidewire too large during cardiac catheterization, resulting in a perforation in the right coronary artery and ultimately death.
Incorrect or Unnecessary Treatment or Procedure Claims
One case included implanting an internal cardiac defibrillator without documented clinical indications, which resulted in a pneumothorax and extended hospitalization.
Another case included placement of a coronary stent with stenosis without documented clinical indications such as the results of the intravascular ultrasound (IVUS).
The Value of Communication
The number of claims that are filed against cardiologists has decreased over the last 14 years. The rate of claims in the last five years seems to indicate that the frequency has leveled off between six and eight claims per 100 FTEs.
The lower rate of claims is an improvement but raises questions about what is needed to reduce the number of patient injuries and the resulting claims even further. One consideration is the percentage of high-severity injuries and death. They have remained stable over the last 13 years. This may be an encouraging statistic considering the increased ages of patients and the increased complexity of procedures. However, efforts to reduce the number of complications and other injuries are needed.
Only 31 percent of claims filed against cardiologists resulted in a payment to the patient or their families. Although it is often difficult to determine the actual cause of undesirable patient outcomes, this statistic seems to indicate that almost 70 percent of claims and suits were not based on negligent care. This raises the question of how to address patients’ concerns and questions so that they do not feel the need to file these claims and suits.
One possible strategy is to closely monitor patient outcomes and identify those with less than desirable results, because patients who have unresolved questions may surmise that undesirable outcomes were due to substandard care. Even with excellent informed consent discussions, it is unlikely that most patients have high enough medical literacy to be able to understand the mechanism of their results. In almost every case, patients need to talk with their cardiologists to understand the reasons for their outcomes. Taking the time to provide explanations will help to satisfy patients’ concerns and build the trust that is needed for successful physician-patient collaboration—which becomes more important, not less, when the patients’ desired outcomes are not able to be achieved.
The guidelines suggested here are not rules, do not constitute legal advice, and do not ensure a successful outcome. The ultimate decision regarding the appropriateness of any treatment must be made by each healthcare provider considering the circumstances of the individual situation and in accordance with the laws of the jurisdiction in which the care is rendered.
11/20