Anesthesiology Closed Claims Study
The Doctors Company has studied anesthesia medical malpractice claims (written demands for payment) since 2007. Our first study involved 640 claims that closed from 2007–2012 and was published in the Journal for Healthcare Risk Management in 2014.
In June 2019, we repeated the study for 587 claims that closed between 2013–2018. The goals for these parallel studies were to determine whether the number of patient injuries had decreased and to identify any new trends in claims involving anesthesia care.
We segregated claims alleging tooth damage (272 claims) and reviewed them separately. Rates of claims and costs of claims (indemnity and expense) were compared between time periods for all anesthesiology claims. Pain medicine claims were also excluded from these studies.
| Study years | All claims | Claims for tooth damage | Claims excluding tooth damage |
|---|---|---|---|
| 2007–2012 | 640 | 144 | 496 |
| 2013–2018 | 587 | 128 | 459 |
| Total | 1227 | 272 | 955 |
Regardless of the outcome, all cases that closed within those time frames were included in this analysis. This approach helps us better understand what motivates patients to pursue claims and gain a broader overview of the individual and system failures and processes that resulted in patient harm.
This study, reinforced by expert insights and relevant case examples, focuses on the following areas:
- Most common case types.
- Most common patient injuries.
- Injury severity.
- Factors contributing to patient injury.
- Strategies for mitigating risk.
Our approach to studying anesthesiology malpractice claims began by reviewing the types of cases represented in these claims to capture the key clinical issues.
We then looked at patients’ injuries to understand the full scope of harm. Physician experts for both the plaintiffs/patients and the defendants/physicians reviewed claims and conducted medical record reviews. They identified factors that caused patients harm and determined whether the standard of care was met. Our clinical analysts drew from these sources to gain an accurate and unbiased understanding of actual patient injuries.
Causes, when known, were attributed to contributing factors. Contributing factor categories include clinical judgment, technical skill, patient behaviors, communication, clinical systems, clinical environments, and documentation.
Our team studied all aspects of these claims and identified risk mitigation strategies that physicians can use to decrease the risk of injury, thereby improving the quality of care.
Anesthesiology Claim Frequency and Cost
Anesthesiology has led other specialties in reducing the risk of harm to patients since the mid-1980s, when the Anesthesia Patient Safety Foundation (APSF) was founded. Since then, clinical practice guidelines have been published by APSF and the American Society of Anesthesiologists (ASA), which have standardized some aspects of anesthesia practice.
Expectations are high to make administration, management, and monitoring of anesthesia safer because of the significant improvements to care with pulse oximetry, capnography, ultrasound-guided central line placement, transesophageal echocardiogram (TEE) monitoring, screening for obstructive sleep apnea, airway classifications, and patient health classifications.
The frequency of claims, including lawsuits, filed against anesthesiologists stayed the same for nine years (2005–2013). A small decrease in the rate of claims, between 1 and 2 percent, occurred in 2014 and in 2015. The decrease in the rate for the 14 years was less than 3 percent.
When compared to the reduction in the number of claims filed per 100 FTEs in other specialties, the percent reduction for anesthesiologists was very small. Even if we associate fewer claims with fewer patient injuries, the best that can be said is that there has been only slight improvement.
Rates of Anesthesiology Claims per 100 FTEs
Historically, the frequency of anesthesiology claims has been lower than most other physician specialties. The rate of claims for anesthesia are better when compared to three other clinical specialties. However, other specialties are gradually reducing the frequency of claims while anesthesiology has remained between 3 and 6 percent for more than 14 years. For example, since 2011, the rate of claims for internal medicine physicians matches that of anesthesiologists.
Rates of Claims by Specialty per 100 FTEs
Anesthesiology
Cardiology
Internal medicine
General surgery
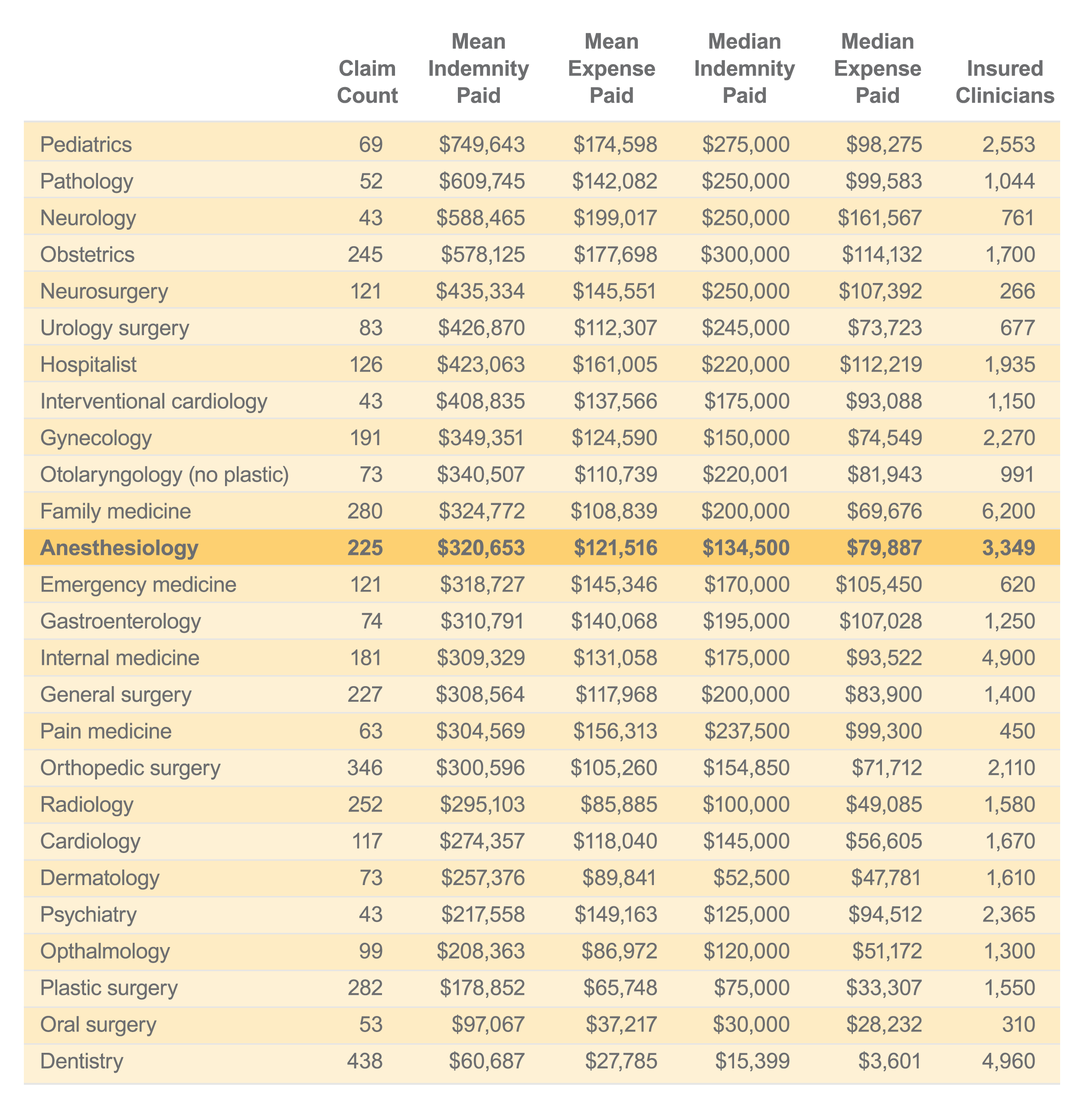
Anesthesiology mean indemnity was 12th out of 25 clinical services between 2013 and 2018. These rankings are based on the average indemnity for all anesthesiology claims compared with the average indemnity for other clinical services insured by The Doctors Company that had more than 40 claims that closed between 2013 and 2018.
Clinical services with 40 or more paid claims sorted by mean indemnity 2013–2018:
Anesthesiology Clinical Service Chart
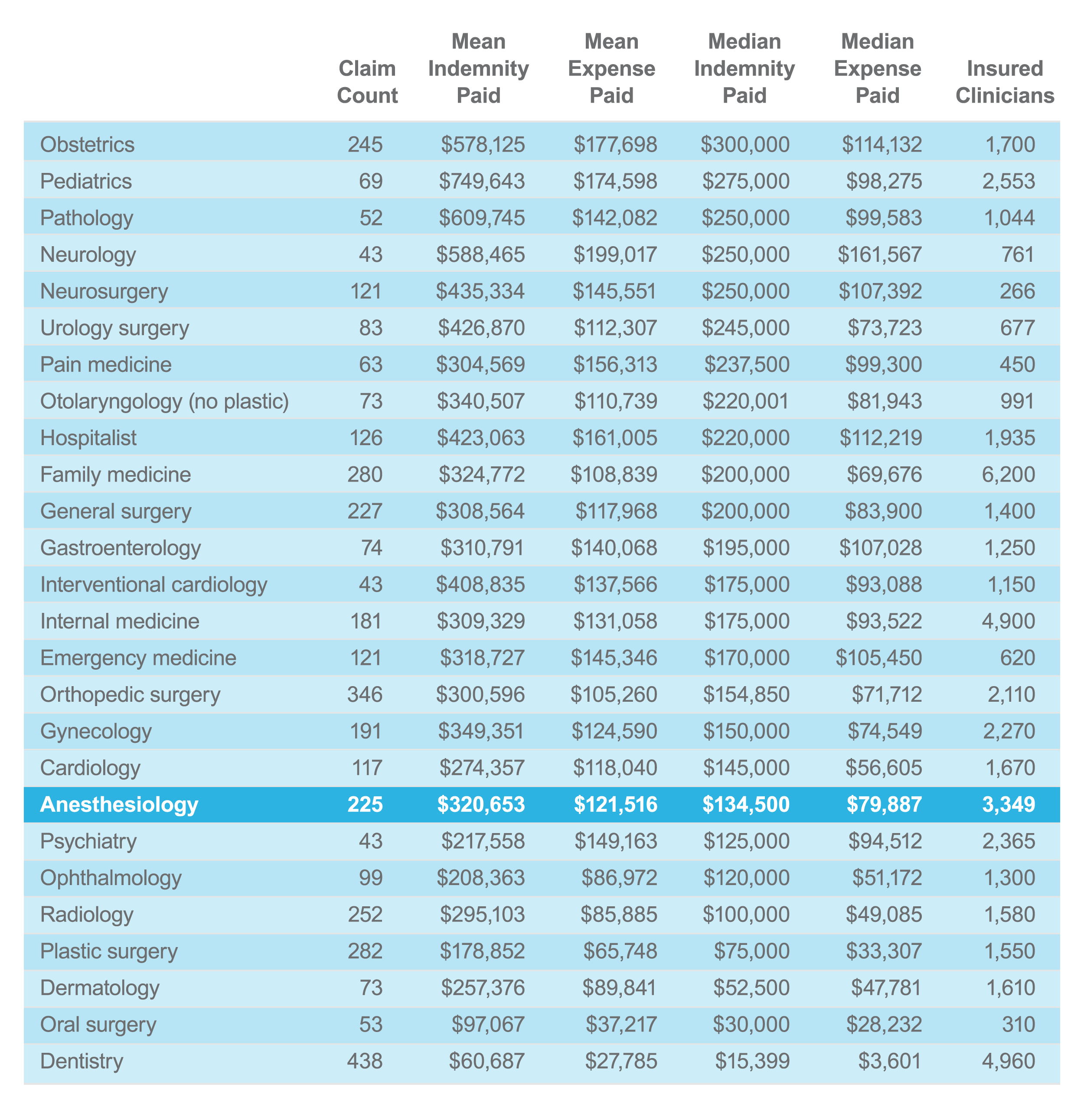
Anesthesiology median indemnity was 19th out of 25 clinical services between 2013 and 2018.
Clinical services with 40 or more paid claims sorted by median indemnity 2013–2018:
Anesthesiology Clinical Service Chart
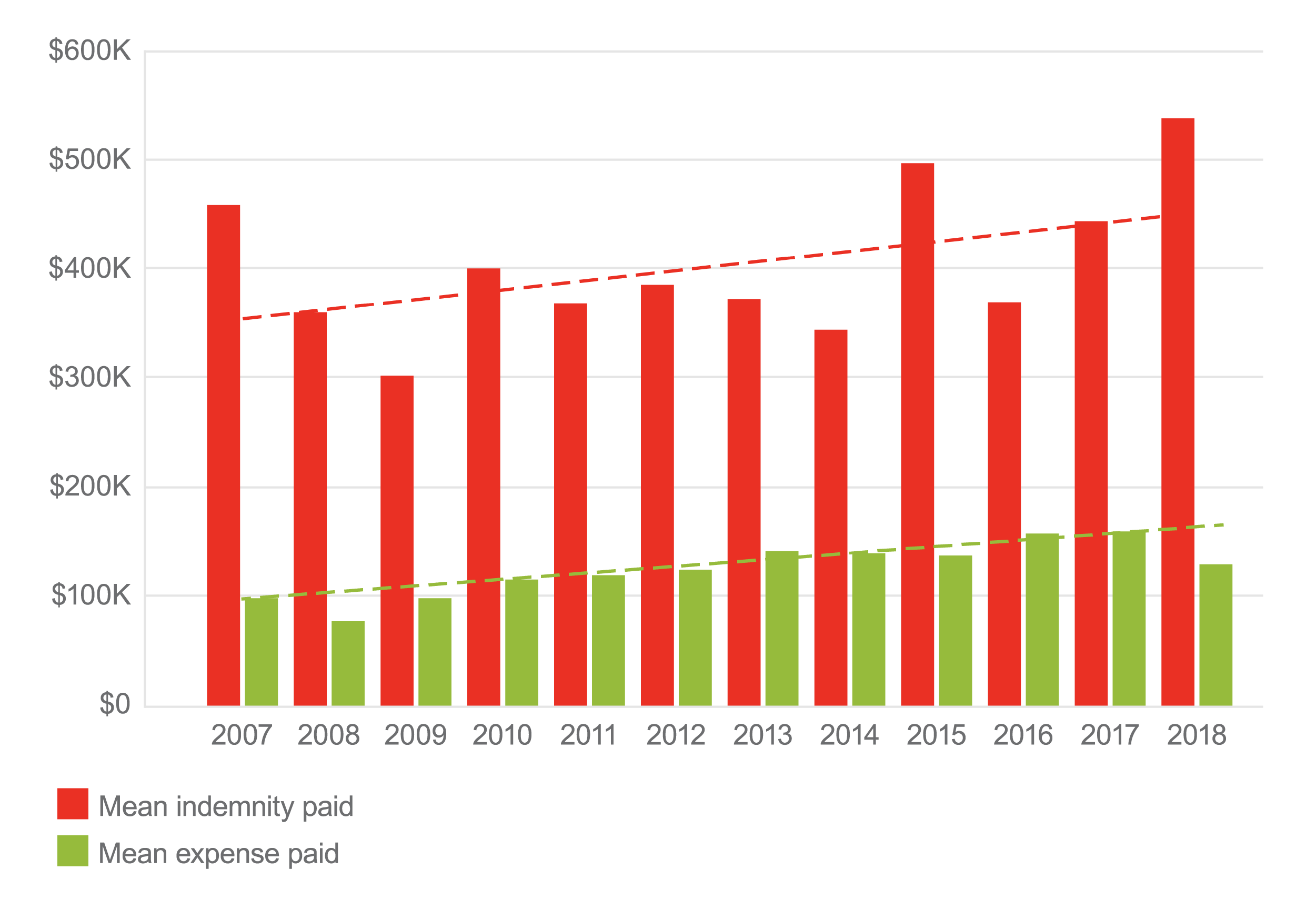
When viewed by year, mean and median indemnity for anesthesiology claims fluctuated significantly.
Mean Indemnity and Expense for Paid Anesthesiology Claims by Assert Year
Mean indemnity paid
Mean expense paid
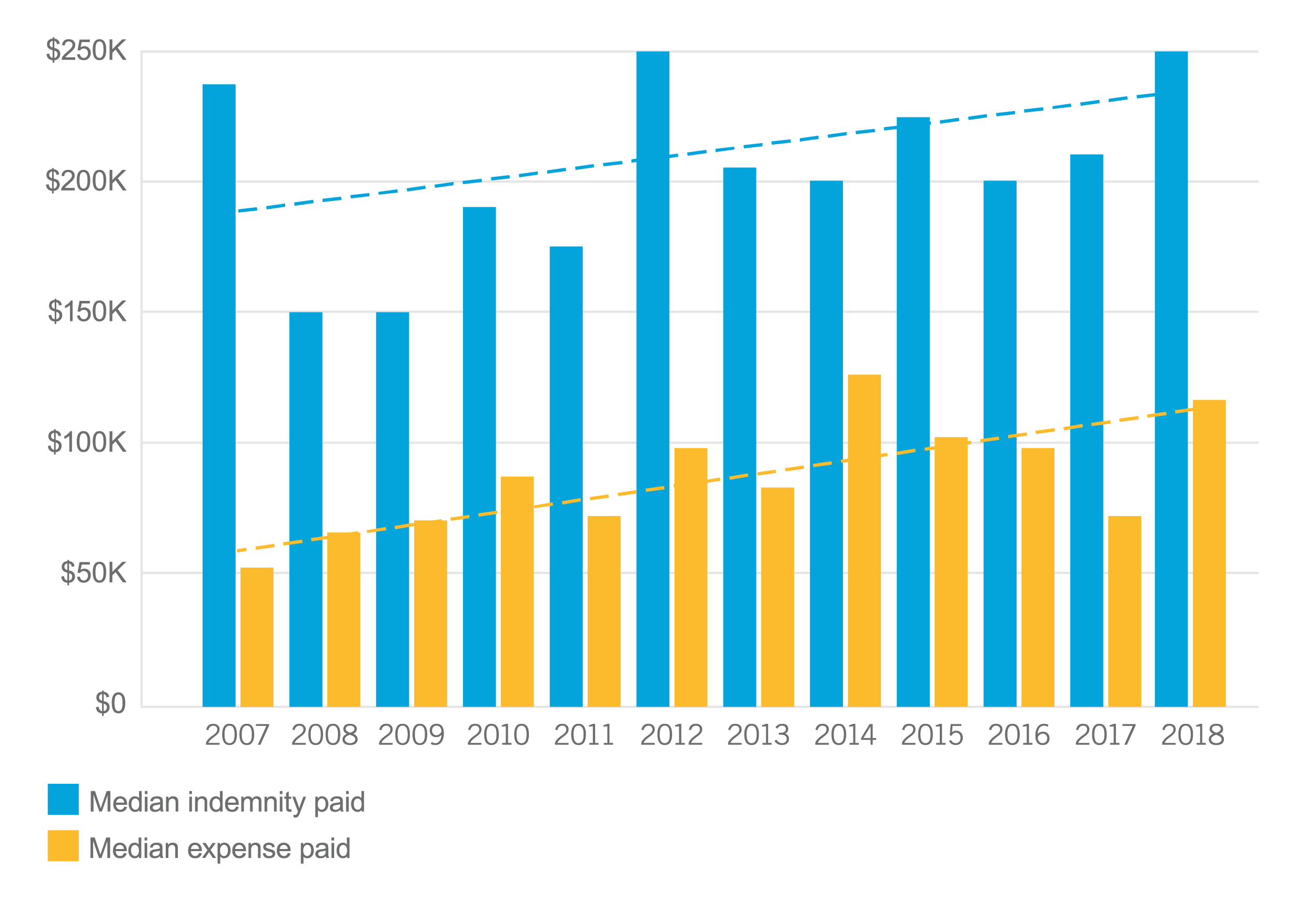
Mean and Median Indemnity for Paid Anesthesiology Claims by Assert Year
Mean indemnity paid
Median indemnity paid
Anesthesiology Tooth Damage Claims
Tooth damage claims continue to make up almost a quarter of all anesthesiology claims (22 to 23 percent). Although tooth damage claims are less expensive than most other types of anesthesia-related injuries, their processing and handling costs can impact the cost of medical malpractice insurance.
Tooth damage claims as a percentage of all anesthesiology claims:
22.5%
of all anesthesia claims
2007–2012
21.8%
of all anesthesia claims
2013–2018
Rate of paid tooth damage claims:
33.3%
of tooth damage claims
2007–2012
30.5%
of tooth damage claims
2013–2018
Mean indemnity for paid tooth damage claims:
$5,693
2007–2012
$2,634
2013–2018
Median indemnity for paid tooth damage claims:
$2,034
2007–2012
$1,760
2013–2018
Mean expense for paid tooth damage claims:
$9,235
2007–2012
$3,894
2013–2018
Median expense for paid tooth damage claims:
$1,788
2007–2012
$321
2013–2018
Tooth damage claims are ubiquitous in situations where intubation is necessary. The numbers captured in our system are not fully representative of all tooth damage claims experienced by the physicians and organizations insured by The Doctors Company. Some groups and organizations choose to adjudicate these claims without submitting them to their professional liability insurance company.
Some patients have anatomy that creates challenges to intubation and other patients have poor dentition. It is essential to evaluate patients preoperatively to determine their dental condition and airway challenges. Plan for airway techniques least likely to damage teeth at risk. In cases of short neck, overbite, limited neck extension, and other anatomical challenges, anesthesia professionals can take precautions against tooth damage. In case of poor dentition and severe gum recession, patients need to be aware of risks to their teeth.
Factors that Contributed to Tooth Damage
In most tooth damage cases, documentation indicated that patients were informed of the risk of tooth damage. The injury was known to the patient as a risk of the procedure (84 percent). In only 3 percent of tooth damage cases was poor technique identified.
The other primary factor determining the outcome of these cases was documentation (13 percent). The two areas of inadequate documentation were lack of descriptive preoperative clinical findings related to dentition, airway, and anatomy and informed consent listing tooth damage as a risk.
According to claims specialists, defense of tooth damage claims is more likely to be successful when anesthesia professionals document the preoperative condition of patients’ dentition, record descriptions of airways, and choose an appropriate intubation process.
Anesthesiology Claims Excluding Cases with Tooth Damage
More than one in five anesthesia claims (22 to 23 percent) allege tooth damage. For this reason, we segregated tooth damage claims from all other anesthesia claim types to provide clear insights to the other anesthesia patient management issues.
| Anesthesiology tooth damage claims | Claims and suits excluding teeth damage claims | Paid claims | Percent of claims with payments |
|---|---|---|---|
| 2007–2012 | 496 | 145 | 29.2% |
| 2013–2018 | 459 | 164 | 35.7% |
In cases excluding tooth damage, mean indemnity and expense increased by 12.5 percent and 36.0 percent respectively between the two time periods included in this study.
Anesthesiology claims mean indemnity for paid claims:
$373,593
2007–2012
$420,250
2013–2018
An increase of $46,657 (12.5 percent)
Anesthesiology claims mean expense for paid claims:
$105,868
2007–2012
$143,979
2013–2018
An increase of $38,111 (36.0 percent)
Median indemnity did not increase when the two time periods were compared. However, median costs for defense (expense) of anesthesiology claims increased by 37.1 percent.
Anesthesiology claims mean indemnity for paid claims:
$200,000
2007–2012
$200,000
2013–2018
An increase of $0.00 (0 percent)
Anesthesiology claims mean indemnity for paid claims:
$70,442
2007–2012
$96,599
2013–2018
An increase of $26,157 (37.1 percent)
When tracked by year, trend lines for mean and median indemnity and expense have increased over time.
Mean Indemnity and Expense for Anesthesiology Claims by Year
Median Indemnity and Expense for Anesthesiology Paid Claims by Year
The trend for more expensive anesthesia claims and suits continues. In 2009, only 19 percent of claims resulted in payment greater than $500,000, but by 2018, this category rose to 36 percent of anesthesiology claims. Most anesthesiology claims remain in the $1 to $499,000 range but the percentage of claims in this category decreased over the last 12 years, from 81 percent in 2009 to 64 percent in 2018.
Anesthesia Claims by Value Range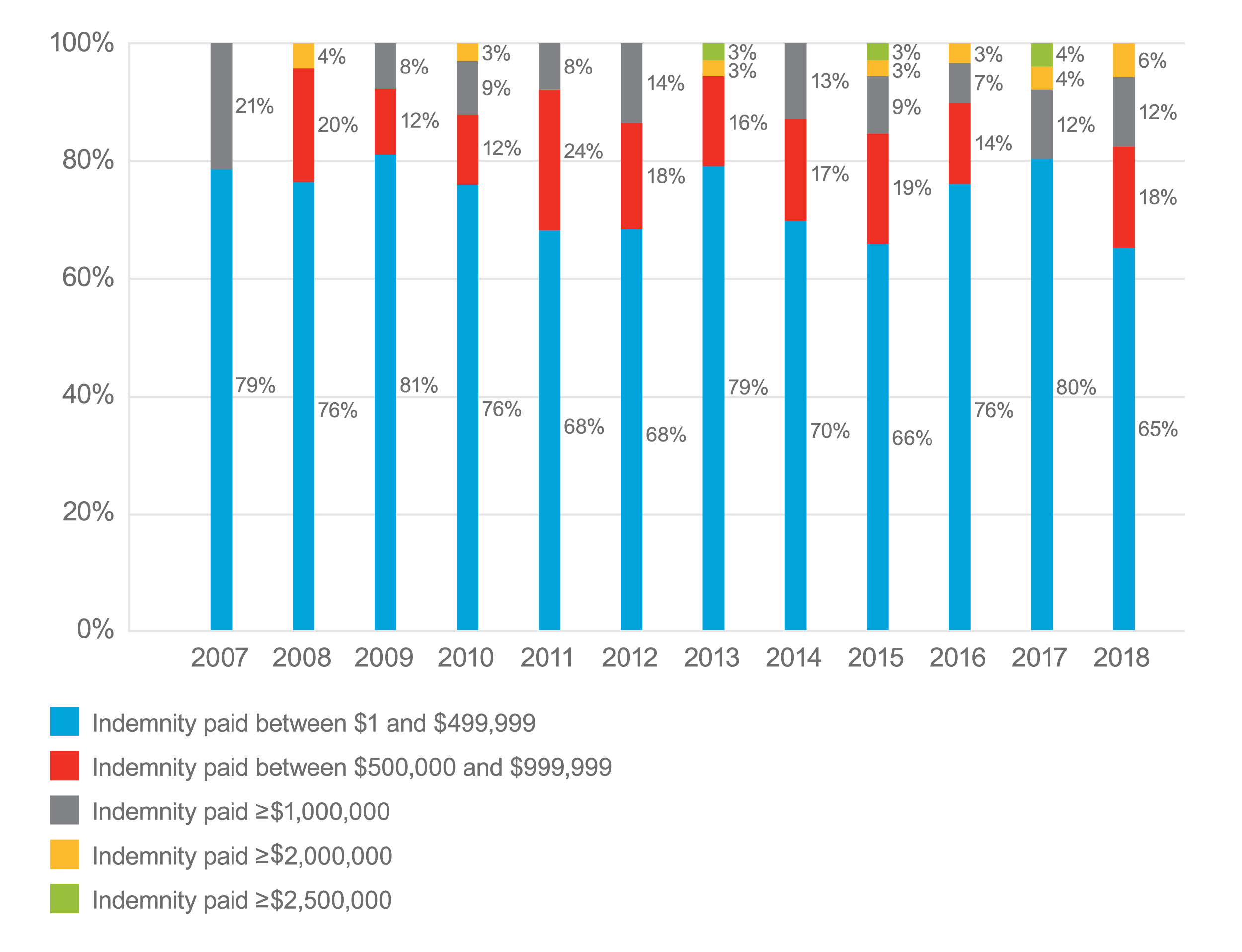
Anesthesiology Injuries Excluding Tooth Damage
The second study found the same types of injuries and at the same percentage of claims as in the first study. Along with a slight decrease in the frequency of anesthesiology claims, it appears that even with the introduction of new technology in recent years, the safety of anesthesia care has not changed in more than a decade. Maybe technology is not the only area where improvements can be made.
Note that the number differences may not be statistically significant. Also, patients may suffer more than one injury so the total is greater than 100 percent.
Top 10 Anesthesia Patient Injuries
| Injury | Claim count 2007–2012 | Percent of total 2007–2012 | Claim count 2013–2018 | Percent of total 2013–2018 |
|---|---|---|---|---|
| Death | 113 | 23% | 107 | 23% |
| Cardiac or respiratory arrest | 68 | 14% | 87 | 19% |
| Organ damage* | 80 | 16% | 84 | 18% |
| Nerve damage | 85 | 17% | 77 | 17% |
| Ongoing pain | 64 | 13% | 63 | 14% |
| Need for surgery | 36 | 7% | 45 | 10% |
| Adverse reaction | 48 | 10% | 39 | 8% |
| Puncture or perforation | 33 | 7% | 39 | 8% |
| Sensory impaired | 31 | 6% | 33 | 7% |
| Mobility dysfunction | 38 | 8% | 32 | 7% |
*In 2007 through 2012, 98 percent of organ damage claims were brain injuries. In 2013 through 2018, 93 percent of organ damage claims were brain damage injuries.
Comorbidities in Anesthesiology Claims Excluding Cases of Tooth Damage
Across anesthesia claims (excluding tooth damage claims) there was not much change in the percentage of claims where these comorbidities impacted the patients’ clinical results. The greatest increase was seen in hypertension, from 3 percent in the earlier study to 9 percent in the 2013–2018 study.
However, there was a sizable impact of comorbidities—patients who suffered harm as a result of improper anesthesia management during surgery—when compared to all other anesthesia claims.
| 2011–2012* | 2013–2019 | |
|---|---|---|
| No comorbidity impact on outcome of care | 71% | 59% |
| Obesity | 19% | 19% |
| Hypertension | 3% | 9% |
| Cardiovascular disease | 5% | 7% |
| Diabetes | 4% | 6% |
| Smoking | 4% | 5% |
| Obstructive sleep apnea | 2% | 5% |
*Note that coding of comorbidities in medical malpractice claims began in 2010 (partial year) so studies of comorbidities began in 2011.
Most Frequent Anesthesiology Case Types Excluding Tooth Damage
The three most common case types made up 63 percent of anesthesia claims in 2007–2012 and 65 percent in 2013–2018.
| Anesthesia case types excluding tooth damage | Claim count 2007–2012 | Percent of claims 2007–2012 | Claim count 2013–2018 | Percent of claims 2013–2018 |
|---|---|---|---|---|
| Improper performance of anesthesia procedure | 169 | 34% | 126 | 27% |
| Improper management of patient under anesthesia | 110 | 22% | 145 | 32% |
| Positioning related | 34 | 7% | 29 | 6% |
| Improper management of surgical patient | 31 | 6% | 25 | 5% |
| Improper performance of treatment or procedure | 25 | 5% | 15 | 3% |
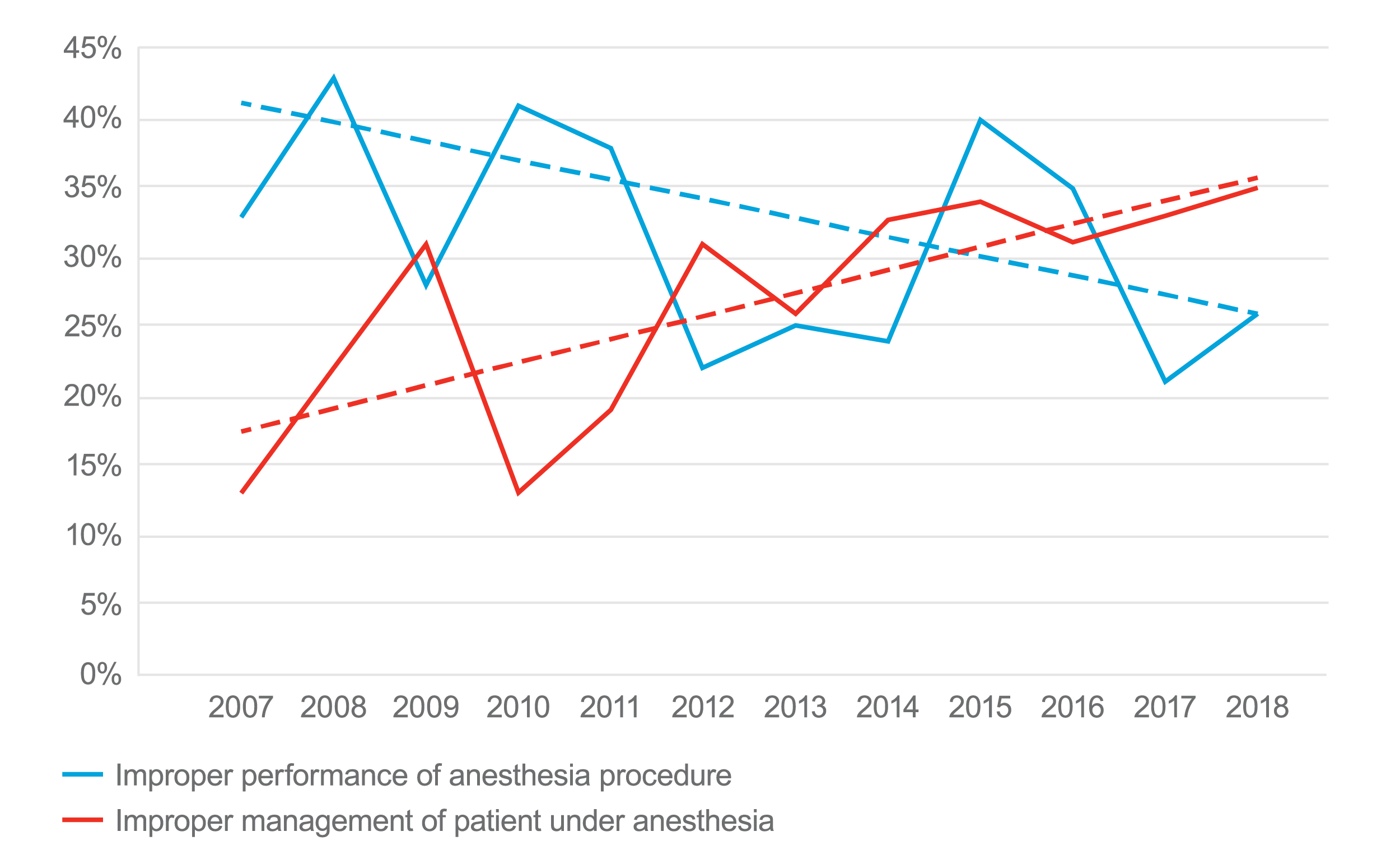
In the first study (2007–2012), improper performance of anesthesia procedure (intubation, injection of anesthesia into a peripheral nerve, injection of anesthesia into spinal canal) was the most common type of claim or suit. It decreased in injuries in the later years. It was proposed at the time that the decline may be due to the introduction of new technologies, like ultrasound-guided regional anesthesia. The downward trend continued in the 2013–2018 study, dropping to 27 percent of anesthesia claims. However, the second study (2013–2018) found that the case type of improper management of patient under anesthesia increased by 10 percent from the earlier study.
Top Two Case Types as a Percentage of Anesthesiology Claims by Year
Twenty-four other case types made up the remaining 37 percent and 35 percent of anesthesiology claims in these two time periods.
Case Type: Improper Management of Patient Under Anesthesia
Claims identified as improper management of patient under anesthesia were due primarily to respiratory, central nervous system, and cardiac complications. These complications were due to comorbidities that were present before the patient was taken to surgery.
Claims of this case type, with inadequate history and physical as a contributing factor, averaged more than two comorbidities per patient. In these cases, 67 percent of the patients had at least one comorbidity. This was two times higher than the percentage of claims with a comorbidity for the rest of the anesthesia cases where only about a third of cases had a comorbidity that impacted the outcome of care.
| Comorbidities for anesthesia claims (excluding tooth damage) including all case types except improper management of patient under anesthesia, 2013–2018 | Percent |
|---|---|
| Obesity | 17% |
| Obstructive sleep apnea | 4% |
| Chronic pulmonary disease | 2% |
| Hypertension | 5% |
| Cardiovascular disease | 5% |
| Renal disease | 2% |
| No comorbidities impacted the outcome of care | 64% |
| Comorbidities for anesthesia claims with the case type improper management of patient under anesthesia (including contributing factor, inadequate history and physical) 2013–2018 | Percent |
|---|---|
| Obesity | 50% |
| Obstructive sleep apnea | 25% |
| Chronic pulmonary disease | 17% |
| Hypertension | 17% |
| Cardiovascular disease | 8% |
| Renal disease | 8% |
| No comorbidities impacted the outcome of care | 33% |
In claims of improper management of patient under anesthesia with inadequate history and physical as a contributing factor, obesity impacted patients’ care in almost three times as many cases as other anesthesia cases. Obstructive sleep apnea was six times more likely to impact the outcome. Hypertension was three times more likely to impact patient’s surgical results. The other comorbidities impacted care outcomes more than twice as frequently.
In these cases, anesthesia providers were managing conditions unrelated to the purpose of surgery but that ultimately were the cause of the patient harm. It appears that many patients were not healthy before surgery started.
Less common comorbidities and other conditions that complicated surgery included clotting disorders (factor 5 mutation), low potassium, interrupted aortic arch, CVA, anticoagulants, asthma, advanced patient age, CHF or COPD, previous damage to airway, MVA and other trauma, pregnancy, and alcoholism.
A review of these cases revealed limited opportunities to conduct preoperative assessments. Older and sicker patients needed closer investigation but production pressures often limited testing and input from attending or referral physicians. These pressures also limited anesthesia professionals’ opportunities to recommend safer locations for anesthesia care (e.g., hospital operating room vs. ambulatory surgery or GI or cardiac labs) or to prepare for complications that might occur as a result of multiple comorbidities or complicated health histories.
Increases in complications and injuries for patients in cases with improper management of patient under anesthesia was also seen in the severity of patient injuries. These patients suffered high-severity injuries in 62 percent of these cases compared with 16 percent of high-severity injuries in all other anesthesiology cases (excluding tooth damage cases).
Percent of Claims 2013 to 2018 with Case Type Improper Management of Patient Under Anesthesia
Percent of Claims 2013 to 2018 Excluding Case Type Improper Management of Patient Under Anesthesia
This highlights the potential for harm in patients with comorbidities and who may not have had adequate history and physical examinations prior to surgery. This data raised the following questions:
- Were the comorbidities known prior to administration of anesthesia?
- Did anesthesiologists and CRNAs have opportunities to adequately assess patients in advance of surgery? Pre-op assessments are important for the anesthesia professional to determine ASA and Mallampati scores and to prepare to handle complications that may result from comorbidities (bleeding, respiratory complications, mean arterial pressures, cardiac conditions).
- Did anesthesia professionals have opportunities to refer patients to specialists to evaluate patients’ comorbidities?
- Did anesthesia professionals take adequate precautions and make adequate preparations before anesthetizing patients with comorbidities?
- Should additional steps be taken prior to surgery for patients who have comorbidities?
Patients may suffer from a wide variety of comorbidities. Some may not be discovered without a thorough history and physical including family history of cardiovascular disease, respiratory conditions, allergies or bleeding disorders.
Other conditions that impacted the outcome of anesthesia care included aspiration of stomach contents; sudden drop in oxygen saturation, blood pressure, and/or heart rate; laryngospasm; and low mean arterial pressures. Anatomical structures like tracheal stenosis and short neck, caused difficult intubations and prone positions caused displacement of endotracheal tubes.
Factors that contributed to patient injuries in the case type improper management of patient under anesthesia included improper selection and management of therapy (44 percent). In most cases, this referred to management of complications that occurred during surgery. Fifty-five percent of these cases had respiratory complications, central nervous system complications, adverse effects of anesthesia, or cardiac complications.
This also referred to the types of anesthesia and the routes of anesthesia that were selected for these patients. Reviewers pointed to patients’ conditions or comorbidities that should have prompted anesthesia professionals to consider other options.
A 56-year-old morbidly obese male with a history of hypertension, diabetes, sleep apnea, and elevated cholesterol presented to ambulatory surgery center for knee arthroscopy. Following a brief pre-op assessment, he was rated as ASA III Mallampati III. It was decided to use LMA with 100 mcg of Fentanyl and 2 mg Versed followed by inhalation anesthesia.
After the procedure, the LMA was removed and the patient was moved to PACU. The patient was unresponsive for about 20 minutes and exhibited signs of respiratory distress. Efforts were made to open the airway with jaw thrusts and nasal trumpet. The anesthesiologist determined that the patient was suffering from congestive heart failure, aspiration, or pulmonary edema.
The anesthesiologist administered 40 mcg of Narcan. The patient began to awaken but had oxygen saturation readings in the high 70s. The patient was encouraged to take slow deep breaths. Rhonchi were heard and the patient complained of shortness of breath. The EKG reading was unchanged from the pre-op test.
Thirty minutes after the first dose, a second dose of 40 mcg Narcan was administered with no improvement. Oxygen saturation remained between 79 and 88 percent. Albuterol was given with little effect. The patient’s respiration rate was 44.
The patient was reintubated. Copious pink frothy fluid was suctioned from the ETT. The patient received Propofol and paralytic agents with the code team present to assist. The patient’s heart rate continued to decline to about 45 beats per minute. The patient was transferred to a hospital emergency department.
Upon arrival in the emergency department, the patient was in asystolic arrest. Attempts to place a transvenous pacer were unsuccessful. The NG tube returned 400 cc of brown coffee-grounds gastric fluid. After 30 minutes of CPR, the patient was pronounced dead.
The autopsy report noted no apparent airway obstruction, so the pathologist determined that the cause of death was flash pulmonary edema. Negative pressure pulmonary edema (NPPE) is a form of flash pulmonary edema caused by forceful inspiratory efforts made against a blocked airway. Toxic levels of ropivacaine were found in the patient’s blood. The pathologist noted hypertrophic cardiomyopathy and grossly enlarged heart.
Plaintiffs argued that the LMA was removed too soon with sleep apnea and a class III Mallampati score. They raised questions about the high levels of ropivacaine and wondered if it contributed to bradycardia. They said that the reintubation took too long resulting in high end-tidal CO2. They also noted inconsistent documentation between PACU nurses and the anesthesiologist.
Some defense experts were supportive of the care, stating that the cause of death was probably from a fatal arrhythmia due to hypotension and enlarged heart. They questioned if undiagnosed pulmonary hypertension would explain the failure to respond to Lasix. It was noted that both of the patient’s parents had died suddenly following surgeries. The assumed cause was coronary artery disease.
The second most common factor for this case type was technical performance. Most of these cases referred to poor technique used in resuscitation and poor technique in intubations.
Patient assessment issues referred to inadequate histories and physicals. As noted above, inadequate H&P had a significant impact on patients with comorbidities. This factor included failure to address abnormal findings and failure or delay ordering diagnostic tests.
A 29-year-old female delivered a baby and then requested tubal ligation that day. Twenty minutes after receiving spinal anesthesia, she began having respiratory difficulty with decreasing oxygen saturation. She was intubated and lung sounds were auscultated but there was no improvement in low end-tidal CO2 levels. She began having seizures and had only a faint carotid pulse.
The outcome was a patient in a persistent vegetative state. Concerns raised by physician reviewers were the delivery day return to surgery because of the higher risk for gastric aspiration. Possible causes included high spinal, bronchospasm, misplaced ETT, and vasovagal response. Following surgery, the surgeon learned that the patient had been ill with an upper respiratory infection for about two weeks.
A 72-year-old male was taken to surgery for a full thickness rotator cuff tear repair. The pre-op assessment was documented with ASA III and Mallampati score of I or II.
Surgery was successful and the patient was transferred to ICU. However, he expired a few days later.
Concerns about his care included poor documentation of the preoperative assessment. The patient had a history of respiratory failure during previous surgeries that required reintubation. In this case, it was determined that the patient had been extubated prematurely in PACU.
Almost all factors related to patient monitoring were for inadequate monitoring of patients’ physiological status. Low mean arterial pressure and severe acidosis resulted in blindness. A drop in end-tidal CO2, likely due to an airway obstruction, was not noted and resulted in encephalopathy and death. Lack of documentation of breath sounds and slow response to drop in CO2 and heart arrhythmia resulted in anoxic brain injury. A patient’s oxygen levels dropped rapidly, and the low pulse oximeter readings were assumed to be due to equipment malfunction. It was later discovered that breathing circuit tubes had disconnected.
A 26-year-old female was taken to surgery for an elbow fracture repair. During surgery, it was discovered that the tourniquet had remained inflated too long, resulting in nerve damage. Plaintiffs raised concerns about the level of monitoring the patient had received during her surgery.
A 71-year-old female received a translumbar epidural steroid injection by a pain management specialist. The anesthesiologist planned to provide MAC, but he delivered propofol in four doses for a total of 350 mg for the short procedure. The patient developed respiratory distress (O2 saturation of 70) and bradycardia (40 bpm). The patient was resuscitated and transferred to ICU.
The outcome was short-term memory loss and loss of emotional control. The patient is unable to perform household chores. Experts raised concerns about the slow response to the patient’s changing status.
A 42-year-old female with a history of asthma, GERD, and BMI of 36 presented with abdominal pain. She was diagnosed with occlusion of cystic duct following a prior cholecystectomy.
The patient was scheduled for an ERCP at the hospital. Her ASA score was 3. The plan for anesthesia was MAC with IV sedation.
A stone was found in the common bile duct. During the procedure, the anesthesiologist was unable to obtain an end-tidal CO2 reading. A second machine was requested but it showed the same reading. The patient began to experience bradycardia (40s) so she was intubated. Her condition continued to deteriorate requiring CPR. A heart rhythm was obtained but the patient did not regain consciousness. She expired several months later.
Reviewers were concerned about the delay in identifying respiratory compromise. They also noted the lack of timely initiation of appropriate resuscitative measures.
A 58-year-old patient with diabetes, BMI of 36, and Stage Five renal failure presented with a necrotic toe. She was admitted for surgery following dialysis. An IV was started in the non-AV-fistula arm, the same arm where her blood pressure was monitored.
When IV anesthesia was administered, the patient’s heart rate dropped into the 60s. The blood pressure monitor was turned off to give additional medications. When the blood pressure monitor was restarted, no blood pressure was readable. The patient’s heart rate dropped into the 30s. The patient was given Atropine, epinephrine, and Phenylephrine.
The patient’s heart rate increased but remained in the 50s, so more medications were given. When surgery was completed, the surgeon left the OR. The patient had no palpable pulse and no pulse oximeter reading.
Chest compressions were initiated, and the patient was intubated. A short time later, the patient had a blood pressure of 130/50, but she did not regain consciousness. Her seizures started a short time later. The patient was moved to ICU where she was diagnosed with diffuse anoxic brain injury. Life support was terminated a short time later and the patient expired.
In the claim brought by the patient’s family, experts on both sides criticized the anesthesia care. There was very limited documentation regarding the patient’s vital signs. The surgeon and the rest of the surgical team were not notified that the anesthesiologist was having difficulty maintaining a reasonable blood pressure.
A 35-year-old female experienced an iliac artery tear during introduction of trocar for laparoscopic hysterectomy. The procedure was converted to open and the artery was repaired. The patient received several units of uncrossed-matched packed red blood cells. The surgery then proceeded.
During the procedure, the patient’s blood pressure continued to drop. The mostly illegible documentation revealed that the patient’s blood pressure moved from being in the 70s to the 50s.
Following the conclusion of surgery, the patient gained some level of awareness but was unresponsive to verbal stimuli. Also, her respiratory rate decreased over the next several hours until she was in respiratory arrest. The patient was resuscitated but a CT scan revealed cerebral edema and brain death.
It was later discovered that the anesthesia professional had not noted the mean arterial pressure that remained below 50 mmHg for more than 30 minutes following the laceration of the patient’s artery. He was also criticized for inadequate care following surgery. It was the sudden respiratory failure following surgery that resulted in cerebral edema and death.
Case Type: Improper Performance of Anesthesia Procedure
In the most recent study, improper performance of anesthesia procedure was the second most common case type, accounting for 27 percent of anesthesia claims. The factor identified most frequently by physician experts as having contributed to patient injury was technical problems that were known risks of the procedure (88 percent of the cases of this type). In these cases, patients were aware of the risks prior to surgery. Only 11 percent of these cases were due to poor technique.
This factor was identified in procedures such as intubation of the respiratory tract (46 percent), injection of anesthesia into peripheral nerve (27 percent), injection of anesthesia into spinal canal (14 percent), and injection of anesthesia into a sympathetic nerve (2 percent). Intubation cases resulted from injuries during intubation or from improperly located endotracheal tubes, causing hypoxia. Injection of anesthesia into spinal canal cases occurred when the injection was incorrectly placed as spinal and not epidural anesthesia.
Injection of anesthesia into a peripheral nerve or peripheral nerve blocks sometimes resulted in nerve damage from inadvertent injection into nerves. The frequency of these cases has decreased in recent years due to the use of ultrasound-guided needle placement. In a few of these cases, it was speculated that the injury came from the tourniquet. As with all cases, lack of or inadequate documentation (18 percent) may have impacted the quality of care and later, the ability of anesthesiologists to defend the care that they provided.
| 1. Technical performance | 88% |
|---|---|
| A. Injury was known to the patient as a risk of the procedure | 77% |
| B. Poor technique | 11% |
| 2. Insufficient or lack of documentation | 18% |
| A. Informed consent | 9% |
| B. Review of participation of care | 5% |
| C. Clinical findings | 3% |
| 3. Selection and management of therapy | 8% |
| A. Invasive procedures | 4% |
| B. Medication related | 2% |
| 4. Communication among providers | 7% |
| A. Regarding patient's condition | 2% |
| B. Information lost in transition of care | 2% |
| C. Failure to read medical record | 3% |
A 55-year-old female was scheduled for hip arthroplasty. She had a history of pulmonary emboli, rheumatoid arthritis including severe arthritis of the left hip. Her preoperative scores were ASA 1 and Mallampati II.
After three attempts to intubate with a MacIntosh rigid blade laryngoscope, the anesthesiologist noted blood in the patient’s mouth. The patient developed laryngospasm and attempts at rapid intubation were unsuccessful. The procedure was canceled.
The patient complained of pain in her neck. She had signs of infection and stridor. A CT scan revealed subcutaneous emphysema and perforation of the hypopharynx. The surgeon ordered an otolaryngology consultation. The patient had a successful surgical repair of the injury to her hypopharynx.
The patient experienced a full recovery but continued to complain of neck pain and difficulty swallowing.
Experts opined that there was an inadequate assessment prior to surgery. There was no evidence that the anesthesiologist reviewed the patient’s medical record. He did not account for the patient’s rheumatoid arthritis-caused stiff and possibly unstable neck and did not attempt to view the patient’s vocal cords. They believed that the inability to see the patient’s vocal cords should have prompted the use of a flexible laryngoscope. The blind attempt to intubate caused the patient’s injury.
A 46-year-old male was taken to surgery for clavicle fracture. The anesthesiologist utilized general anesthesia and a right interscalene block guided by ultrasound.
The surgeon performed an ORIF using fluoroscopy. No complications were noted, and the patient was discharged the same day.
After discharge, the patient experienced numbness in his right arm. The surgeon thought it would resolve. Later it localized as pain and weakness in the right hand. A neurologist diagnosed the patient with incomplete brachial plexus palsy and then brachial plexopathy.
Experts disagreed as to whether the interscalene block was appropriate for this surgical procedure. Some said that the nature of the fracture increased the risk of brachial plexus injury. However, they agreed that documentation was lacking details of the procedure. There was no informed consent discussion regarding the risk of interscalene block. Defense experts believed that scar tissue rather than the procedure caused the problem.
Observations and Summary
- Claims filed against anesthesiologists have historically occurred less frequently than claims experienced by other specialties. However, other specialties have experienced gradually decreasing rates of claims while anesthesiology has remained between 3 and 6 percent of the cases for the last 14 years. This raises the question, what do anesthesia professionals need to do to continue to reduce the frequency with which claims are filed? A study of these claims and suits seems to indicate that inadequate preoperative assessments were a significant factor.
- The mean indemnity for anesthesiology claims placed this specialty 12th out of 25 clinical services in the years 2013–2018. Anesthesiology median indemnity was 19th out of 25 clinical services during those same years.
- Tooth damage claims continue to make up almost a quarter of all anesthesiology claims (22 percent to 23 percent). Although tooth damage claims are less expensive than most other types of anesthesia-related injuries, their processing and handling costs can impact the cost of medical malpractice insurance, and tooth damage is a source of great patient dissatisfaction.
- According to claims specialists, defense of tooth damage claims is more likely to be successful when anesthesia professionals document the condition of patients’ dentition, document airway anatomy, and record the intubation process.
- The trend for higher indemnity in anesthesia claims and lawsuits, continues. Since 2009 when only 19 percent of indemnity payments were greater than $500,000, the percentage of indemnity payments in 2018 that was greater than $500,000 jumped to 36 percent.
- The cost of defense of anesthesia claims continues to increase. The trend lines over the last 12 years shows upward slopes. Both mean and median defense costs increased by more than 36 percent when comparing costs of claims between 2007–2012 and 2013–2018 study years.
- The most common case type in the 2007–2012 study was improper performance of anesthesia procedure. However, in that study, we saw a downward trend over those years for this case type. That finding was borne out in the 2013–2018 study where we found that the case type improper performance of anesthesia procedure dropped by 7 percent and became the second most common case type.
- In the 2007–2012 study, the case type improper management of patient under anesthesia was the second most common. In the 2013–2018 study it was the most common, having increased by 10 percent between the two studies.
- Claims identified as being improper management of patient under anesthesia, were due primarily to respiratory, central nervous system, and cardiac complications. These complications were due to comorbidities that were present before the patient went to surgery.
- Claims with the allegation improper management of patient under anesthesia averaged more than two comorbidities per patient. In these cases, 67 percent of the patients had at least one comorbidity. This was two times higher than the percentage of claims with a comorbidity for the rest of the anesthesia cases where only about a third of cases had a comorbidity that impacted the outcome of care.
Risk Mitigation Strategies
The following strategies can assist physicians and other providers in reducing risk and improving quality of care:
- Include information in informed consent discussions about anesthesia risks including special positioning risks and risks of special procedures like nerve blocks and arterial lines. Patients with dental appliances or poor dentition should be informed of the risks.
- Work with surgeons, proceduralists, and healthcare organizations to ensure adequate time for preoperative assessments and testing. Some anesthesiologists report pressure to proceed with surgery when they have not had time to do more than a cursory review of the patient and his or her history.
- Include a review of the patient’s previous experience with anesthesia in the history and physical. When possible view previous anesthesia records.
- Tailor anesthesia plans for each patient to specifically address any abnormal findings or comorbidities identified during the history and physical.
- Fully document the preoperative anesthesia assessment. In one case discussed in this study, the existence of obstructive sleep apnea should have dictated removal of endotracheal tube or LMA only after the patient was awake and able to respond. Patients with difficult airways should be awake and able to respond to commands before airways are removed.
- After patients are extubated, airways sometimes close due to obstructive sleep apnea, neck swelling, hematomas, laryngospasms, etc. For these reasons, equipment for performing emergency cricothyrotomies or tracheostomies must be immediately available in case attempts to reintubate fail.
- Patients may suffer from a large variety of comorbidities. Some may not be discovered without a thorough family history of cardiovascular disease, respiratory conditions, allergies, or bleeding disorders. Prompt patients to be prepared to discuss family history before presenting for preoperative assessments.
- Even fasting patients may accumulate large amounts of fluid in their stomachs. Caution should be taken when intubating to reduce the chance of aspirating vomit.
- One complication of placing patients in the prone position is inadvertent dislocation of endotracheal tubes. Close monitoring of these patients is important. The surgeon should be notified if there are concerns about respiration rates, end-tidal CO2 levels, oxygen saturation, or any other monitored metric or vital sign.
- Mean arterial pressure is a factor in cases involving bleeding and in cases involving positioning. Patients can suffer brain injury from inadequate oxygenation during surgery if the mean arterial pressure and cerebral perfusion pressure are not maintained within a safe range for each patient.
- The most common procedures in cases of alleged improper performance of anesthesia procedure include intubation of respiratory tract and injection of anesthesia into peripheral nerve, spinal canal, or sympathetic nerve. The most effective defense is good documentation.
- The most common factor that contributed to patient injury was complications of the procedure. These injuries were known to patients as risks of the procedure. Poor technique was found in only about 11% of anesthesia cases. When patients suffer from known complications, create opportunities to talk with patients and/or their families. Patients may not remember informed consent discussions or the content of the consent form document they were provided, and may not understand that the injury that they experienced was known as a risk of the procedure. Help patients understand and offer to answer their questions, thus building trust and providing explanations that patients deserve.
- Decisions about providing care to patients in the appropriate setting is often made by anesthesiology professionals. Pre-op assessments performed at least a week in advance of surgery provide time to schedule patients at an appropriate location where a higher level of care is available if needed.
- Documentation is essential for providing good care and for defending that care, often years after the services were provided.
Rare situations don’t require extensive discussion since anesthesia professionals know how to provide high-quality care. However, the following circumstances from case reviews may be instructive, so they are included here:
- The patient was given a paralytic agent but not anesthetized (failed to turn on the anesthetic gas so there was a period of awareness).
- Records were suspected of being fabricated because they did not fit the clinical picture.
- Burns from radiation or previous surgeries resulting in scar tissue made intubation difficult—not identified in the patient’s history and physical pre-op assessment.
Conclusion
The purpose of this study is to identify those rare circumstances that result in patient harm. Although anesthesia professionals provide excellent care for almost every patient, there is value in seeing those situations where circumstances prevented good care.
Our hope is that this summary of data that arose from medical malpractice claims will serve as a reminder that excellent clinicians can find themselves in situations where they are fighting to save patients’ lives. This data shows that comorbidities can complicate the delivery of good anesthesia care. It reinforces the importance of thorough histories and physicals as a way of identifying potential problems and preparing to address them in the administration of anesthesia care.
References
Ranum D, Shapiro F, Chang B, Urman D. Analysis of patient injury based on anesthesiology closed claims data from a major malpractice insurer. J Healthc Risk Manag. 2014;34(2):31-42
The guidelines suggested here are not rules, do not constitute legal advice, and do not ensure a successful outcome. The ultimate decision regarding the appropriateness of any treatment must be made by each healthcare provider considering the circumstances of the individual situation and in accordance with the laws of the jurisdiction in which the care is rendered.
02/20

