Study of Malpractice Claims Involving Children
The Doctors Company analyzed 1,215 claims (written demands for payment) filed on behalf of pediatric patients that closed from 2008 through 2017. The study is based on the claims filed against physicians in 52 specialties and subspecialties.
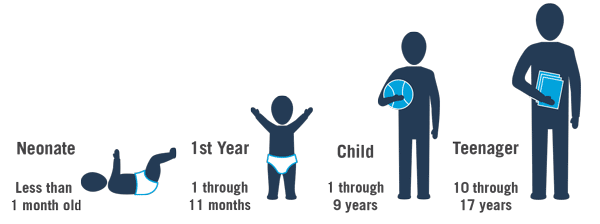
Great developmental differences exist between neonates in their first month of life and teenagers who are ready to enter adulthood—in some cases, having borne children of their own. To identify the differences based on age, we focused on four age groups:
We included all medical malpractice claims and lawsuits against physicians in medical and surgical specialties but excluded dentists and oral surgeons.
Regardless of the outcome, all cases that closed from 2008 through 2017 were included in this analysis—an approach that helped us better understand what motivates patients and families to pursue claims and gain a broader overview of the system failures and processes that resulted in patient harm.
This study provides an overview of the most common types of claims, expert insights into the specific elements that led to patient injury, and risk mitigation strategies.
Our approach to studying these malpractice claims began by reviewing plaintiffs’/parents’ allegations. This provided insights into their understanding of what happened to the child and their motivations for filing claims.
The next step was to catalog patients’ injuries to understand the full scope of harm. Physician experts for both the plaintiffs/parents and the defendants/physicians reviewed claims and conducted medical record reviews. Our clinical analysts drew from these sources to gain an accurate and unbiased understanding of actual patient injuries.
To prevent injuries, it is essential to understand the factors that contributed to patient harm. Categories of contributing factors include clinical judgment, technical skill, patient behaviors, communication, clinical symptoms, clinical environments, and documentation. Physician experts identified factors that contributed to patient harm and evaluated each claim to determine whether the standard of care was met.
Physician Specialties
The pediatric patients in this study were treated by a variety of physician specialties. Obstetricians were most frequently involved with neonatal patients. Pediatricians, orthopedic surgeons, emergency medicine physicians, and family medicine physicians were most frequently named as defendants in claims filed on behalf of children older than one month of age.
The top 10 physician specialties named as defendants represented 72 percent of all pediatric patient claims:
Pediatric Claim and Lawsuit Payments
Of the 1,215 claims in the study, 446 (37 percent) resulted in a payment to the claimant.
$630,456
Mean indemnity
payment
$157,592
Mean expense
paid
The median indemnity payment was $250,000, and the median expense to defend these claims was $99,984.
A review by age group showed that neonates had the highest mean indemnity ($936,843) and median indemnity payment ($300,000). The mean expense was also the highest ($187,117), as was the median expense ($119,311).
Pediatric age group categories for paid claims:
| Mean indemnity paid | Mean expense paid | Median indemnity paid | Median expense paid | |
|---|---|---|---|---|
| Neonate | $936,843 | $187,117 | $300,000 | $119,311 |
| First year | $448,205 | $150,570 | $200,000 | $117,882 |
| Child | $493,100 | $146,060 | $200,000 | $94,174 |
| Teenager | $386,849 | $129,816 | $162,500 | $83,205 |
| Claim count | Percent of claims with indemnity | |
|---|---|---|
| Neonate | 173 | 39% |
| First year | 33 | 34% |
| Child | 108 | 37% |
| Teenager | 132 | 35% |
The median number may be a more accurate representation of the amount of indemnity in paid claims. The median eliminates the impact of very high or very low indemnity amounts, giving a better idea of a typical value.
Although there are some differences between the mean and median amounts of indemnity paid in pediatric patient claims, the percentage of claims that are paid for each patient age group is very similar.
Long-Term Claim Exposure
A concern often raised regarding the care and treatment of pediatric patients is that minors and their representatives can file claims many years after treatment is provided.
Our pediatric study looked at the length of time from the event that caused the alleged patient harm until the claim was filed.
We learned that 76.7 percent of the claims were filed within three years of the event. By five years, 85.1 percent of claims had been filed; by 10 years, 96.7 percent of claims were filed. Only 1.9 percent of pediatric claims were filed 11 through 15 years after the patient was harmed, and only 1.1 percent of pediatric claims were filed 16 through 20 years after the event.
Our experience indicates that 3 percent of pediatric claims were filed more than 10 years after the injury. This highlights the importance of quality documentation. Years after the alleged harm, it is still a factor in defending claims.
Years from event until claim was filed:
Treatment Locations
Pediatric patients were treated in a variety of locations. Neonates were most often treated in labor and delivery (60 percent) and a physician’s office or clinic (14 percent). Children in their first year were most often treated in a physician’s office or clinic (45 percent) or a hospital room (14 percent). Children ages one through nine years received most treatment in their physician’s office or clinic (37 percent) or in the emergency department (14 percent). Teenagers received their care most often in a physician’s office or clinic (40 percent), ambulatory surgery (16 percent), and emergency department (12 percent).
Location where care was provided:
| Neonates | First year | Child | Teenager | |
|---|---|---|---|---|
| Physician office or clinic | 14% | 45% | 37% | 40% |
| Labor and delivery | 60% | 3% | 0% | 4% |
| Emergency department | 2% | 11% | 14% | 12% |
| Ambulatory surgery | 1% | 1% | 11% | 16% |
| Hospital operating room | 2% | 6% | 9% | 10% |
| Patient's hospital room | 2% | 14% | 7% | 7% |
| Nursery | 9% | 2% | 0% | 0% |
| Neonatal ICU | 7% | 2% | 0% | 0% |
| Pediatric ICU | 1% | 5% | 4% | 2% |
| Patient's home | 0% | 3% | 6% | 0% |
| Radiology | 1% | 2% | 3% | 2% |
Most Commonly Injured Body Parts
The most common neonatal patient injuries were:
Patients in their first year of life suffered injuries to:
Patient deaths occurred in 13 percent of claims filed for neonatal patients, 30 percent for patients in their first year of life, 15 percent for children ages one through nine, and 13 percent for teenaged patients.
Children ages one through nine most commonly suffered injuries to:
Teenagers most commonly suffered injuries to:
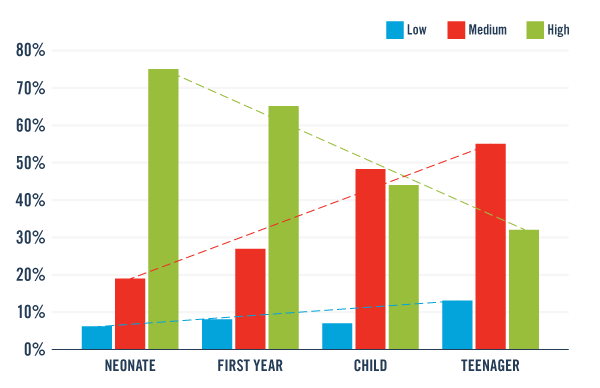
Injury Severity
Patient injury severity varies by age group. Younger patients suffer high-severity injuries at a higher rate (neonate: 75 percent; first year: 65 percent) compared with older patients (child: 44 percent; teenager: 32 percent).
Most Common Patient Allegations
Studying allegations clarified the motivations for filing claims. In outlining the allegations for each group, we included categories of allegations totaling 3 percent or more.
The most common allegation for neonates was obstetrics-related treatment for injuries that occurred during labor and delivery (63 percent). Other age groups had few cases related to obstetrics-related treatment.
Most common allegations for neonate age group (<1 month):
| Number of claims | Percent | |
|---|---|---|
| Obstetrics-related treatment | 283 | 63% |
| Diagnosis-related (failure, delay, wrong) | 62 | 14% |
| Medical treatment (nonobstetric) | 58 | 13% |
| Surgical treatment (nonanesthesia) | 17 | 4% |
For patients in their first year of life, 3 percent of the cases included allegations related to obstetrical treatment.
Most common allegations for first-year age group (1 to 11 months):
| Number of claims | Percent | |
|---|---|---|
| Diagnosis-related (failure, delay, wrong) | 44 | 44% |
| Medical treatment (nonobstetric) | 21 | 21% |
| Surgical treatment (nonanesthesia) | 7 | 8% |
| Patient monitoring | 3 | 3% |
| Obstetrics-related treatment | 3 | 3% |
| Anesthesia-related treatment | 3 | 3% |
| Failure to warn of risks | 3 | 3% |
| Failure to provide safety (falls) | 3 | 3% |
| Other medication-related | 3 | 3% |
For children ages one through nine, less than 1 percent of cases involved obstetrical care.
Most common allegations for child age group (1 to 9 years):
| Number of claims | Percent | |
|---|---|---|
| Diagnosis-related (failure, delay, wrong) | 112 | 38% |
| Medical treatment (nonobstetric) | 64 | 22% |
| Surgical treatment (nonanesthesia) | 52 | 18% |
| Communication (other) | 19 | 6% |
| Improper medical management | 11 | 4% |
Obstetrics-related allegations for the teenager group made up 3 percent of the claims. All 13 of the teenager group claims with an obstetrics-related allegation involved a pediatric patient who was pregnant and received care during pregnancy, labor, and delivery.
Most common allegations for teenager age group (10 to 17 years):
| Number of claims | Percent | |
|---|---|---|
| Diagnosis-related (failure, delay, wrong) | 128 | 34% |
| Surgical treatment (nonanesthesia) | 89 | 23% |
| Medical treatment (nonobstetric) | 73 | 19% |
| Improper medical management | 22 | 6% |
| Anesthesia-related treatment | 14 | 4% |
| Obstetrics-related treatment | 13 | 3% |
Diagnosis-related allegations were the most common allegation in all but the neonate age group. Age groups older than neonates experienced diagnosis-related claims in 34 to 44 percent of all claims and lawsuits in their age group.
In the neonate age group, cases with a diagnosis-related allegation included ventricular septal defect, kernicterus, hydronephrosis, congenital deformity of the hip, and infections (sepsis, group B strep, and enterocolitis, for example).
A female infant was born with Down syndrome. The patient’s pediatrician ordered a cardiology consult after hearing a murmur the second day of life. An echocardiogram was performed the same day. Two days later, it was interpreted as being significantly abnormal and requiring a cardiology consult and further imaging.
The cardiologist dictated the report and faxed it to the hospital. He did not, however, contact anyone at the hospital to confirm that the report had been received. The murmur seemed to resolve, so the patient was discharged home.
Two days after discharge, the patient was seen for a follow-up visit for slight jaundice. No murmur was detected at that time.
Ten days later, the patient was seen by her pediatrician. According to hospital personnel, the echocardiogram report was still not available. One month later, the patient received immunizations but was not evaluated by her pediatrician. The echocardiogram report was still not available.
The parents relocated and did not return to the baby’s original pediatrician. The patient reportedly failed to thrive and died at home. An autopsy revealed the same cardiac abnormalities reported by the cardiologist.
When the original pediatrician was notified that the baby had expired, he reviewed the chart and found that the echocardiogram report had never been received. When he called the hospital, staff had difficulty locating the report because it had been filed with the mother’s record.
The parents filed a claim. Experts felt the patient would have had a good chance of survival if the defect had been surgically repaired. Experts were critical that the pediatrician failed to follow up on the echocardiogram report he had ordered. They also criticized the cardiologist for not verbally communicating the abnormal results and the hospital for mishandling the report. The attending physician who took over the patient’s care following the parents’ relocation had a duty to request medical records from the hospital and from the pediatrician who first treated the patient.
In older age groups, the most common diagnoses in cases with a diagnosis-related allegation included fractures and dislocations, malignant neoplasms (brain, mediastinum, eye, genital organs, skin, lymph nodes, etc.), torsion of testis, meningitis, pneumonia, acute appendicitis, viral and bacterial infections (MRSA and septicemia, for example), and cardiac conditions.
A four-year-old male was seen by an ophthalmologist for intermittent right eye esotropia. Following a dilated exam, the patient was diagnosed with amblyopia and hyperopia. Treatment was corrective lenses and an eye patch two hours per day to strengthen the right eye. A follow-up appointment was recommended in two months.
Several months later, the patient was seen by a second ophthalmologist who agreed with the first diagnosis and treatment.
At the four-month follow-up appointment, the patient appeared to be doing better with the use of the patch and vision exercises. Dilation examinations were performed.
Four months later, the patient’s eyes appeared cosmetically to be straight. There were no neurological signs, but the patient’s vision was worse. The physician recommended continuing with the same treatment.
Approximately three months later, the patient presented to his pediatrician with complaints that his vision was worse and that he was unable to see at times. He experienced headaches and vomiting. The pediatrician referred him to a neurosurgeon to rule out a brain tumor.
Five days later, and prior to the consultation with the neurosurgeon, the patient was taken to the ophthalmologist with complaints that he could not see with both eyes for a short time. He also reported headaches with vomiting. The dilated exam revealed papilledema of the left optic nerve and mild atrophy of the right optic nerve.
The neurosurgeon immediately ordered an MRI and planned to admit the patient to the hospital. The MRI revealed a midline tumor astrocytoma just above the optic chiasma with hydrocephalus. A first surgery biopsied the tumor and relieved the hydrocephalus. A second surgery removed the tumor.
Postoperatively, the patient suffered a stroke with left hemiplegia and affected speech. The patient is now blind in his left eye. He requires braces on his hand and foot and receives therapy for cognitive and physical deficits.
Experts expressed differing opinions. One opined that the standard of care would have been to order an MRI when the patient’s vision changed. The second said that an MRI is not always indicated for strabismus but should have been ordered for sixth nerve palsy. The same expert stated that if the ophthalmologist had done a second dilated exam when the patient’s vision changed, he may have identified papilledema sooner. The third expert said that an earlier diagnosis of this slow-growing tumor would not have changed the risk of stroke from surgery.
Allegation Trends
A review of allegations for neonatal patients over a 10-year period showed a general decrease in allegations of delay in treatment of fetal distress until it increased again in 2015 and 2016. Allegations of improper performance of vaginal delivery (including brachial plexus injuries from shoulder dystocia, brain damage from forceps, and vacuum-assisted deliveries) have decreased as a percentage of neonatal claims since a high in 2011. Improper management of treatment allegations increased from 0 in 2008 to 25 percent in 2015; then the allegations peaked again at 24 percent in 2017. Examples of improper management of treatment included management of sepsis, subgaleal hematoma, respiratory distress, and anemia and bilirubinemia.
Allegations in claims for neonate age group (<1 month):
Delay in treatment of fetal distress
Improper performance of vaginal delivery
Diagnosis-related (failure, delay, wrong)
Improper management of treatment
The neonate was delivered vaginally at 36 weeks by vacuum assist after one pull. There were no pop-offs. The mother had been admitted to labor and delivery due to more than 12 hours of leaking fluid. She was induced and then assisted with the delivery due to exhaustion.
The infant’s head had an abrasion along the vacuum line on the scalp along with caput succedaneum. The head appeared to be diffusely swollen.
The neonate was admitted to the neonatal intensive care unit (NICU) under the care of a neonatologist. The patient was mottled and hypotonic with a low hemoglobin of 10.8 g/dL (normal range 15–20 g/dL). The physician suspected subgaleal hemorrhage and suggested a blood transfusion. The parents refused for religious reasons.
The physician ordered an antibiotic and an ultrasound for the following morning. He planned to monitor the patient’s hemoglobin.
That afternoon, the nurses recorded the gradually increasing caput. They were unable to palpate sutures due to edema. Blood pressure was normal. That night, nurses noted abnormal movements along with increasing head circumference and caput size. Nurses called the neonatologist and reported abnormal movements and increasing head circumference.
At 5:00 AM, the nurse received a call from the laboratory stating that the patient’s hemoglobin was 8.9 g/dL. She called the neonatologist, who ordered STAT laboratory tests and an electroencephalogram. At 10:40 AM, the patient was transferred to a larger hospital.
The assessment of the receiving neonatologist indicated that the neonate was critically ill with profound hypovolemic shock and metabolic acidosis. An ultrasound indicated no intracranial hemorrhage, but an MRI showed profound hypoxic ischemic encephalopathy. The child has microcephaly, profound intellectual disability, cortical visual impairment, seizures, and profound spastic quadriplegia.
Experts opined inadequate management of the subgaleal bleeding and caput succedaneum. Fluid resuscitation was insufficient for the worsening problem. Nurses should have notified the neonatologist of the expanding head measurements, and the neonatologist should have examined the patient when abnormal movements were reported. The neonatologist should have ordered an urgent neurological consult.
For pediatric patients other than neonates, allegations related to diagnosis (failure, delay, or wrong) have remained high each year, ranging from 29 percent to 47 percent over 10 years. The most common examples included torsion of testis, acute appendicitis, meningitis, pneumonia, fracture of epiphysis, benign neoplasm of the brain, dislocated elbow, spotted fevers, cardiac arrest, osteomyelitis of pelvic bones, slipped femoral epiphysis, congenital deformity of the hip, and postoperative infection.
Improper management of treatment, the second-most common allegation for this age group, varied from 5 percent to 16 percent over 10 years. Examples of improper management of treatment in patients older than neonates included management of pneumonia, meningitis, sickle cell trait, and fractures.
Allegations in claims for pediatric patients (excluding neonates):
Diagnosis-related (failure, delay, wrong)
Improper management of treatment
Improper performance of surgery
Improper performance of treatment or procedure
A 16-year-old male was playing football when he received a helmet-to-helmet tackle. A second player hit his head and neck.
The team physician sidelined the player but did not believe that he had a concussion. The player did not lose consciousness or exhibit signs of confusion. The physician believed that the player may have suffered a pinched nerve due to sensations radiating down his arm.
Four days later, the player saw his family physician. He reported taking ibuprofen for neck pain, neck muscle spasms, and headache since the injury. He denied experiencing nausea, vomiting, visual abnormalities, amnesia, or difficulty thinking clearly.
He was diagnosed with a grade-one concussion with a primary complaint of neck muscle spasms. The physician discussed the benefits of a CT scan, but the family refused due to lack of insurance. There was no documentation of this conversation.
The plan was to treat the patient/player with ibuprofen and to not play football for one week. He was told he could return to playing when his symptoms were completely resolved.
A week later, the patient told his mother that the headaches were gone. She called the physician, asking him to sign a release for her son to return to playing football. The physician signed the form but did not reexamine him.
He played in a game that evening and suffered another hard hit during the game. He exhibited slowed reflex times and seemed confused. When the patient suffered another hard hit, he walked to the sideline and collapsed.
He was transported from the field to a hospital, where a CT revealed an acute subdural hemorrhage. He was taken to surgery to drain the hematoma but suffered rapid brain edema and expired.
Experts differed on the care he should have received. One stated that the physician should have reexamined the patient before clearing him to return to playing football. The coach should have removed him from the game when he exhibited signs of confusion.
A second expert believed that a second assessment was not required, but a third physician reviewer believed that the patient should have been evaluated a second time. Another opined that the patient should have been sidelined for a week after the symptoms subsided.
The differences of opinion hinged on the cause of the injury. Experts disagreed on whether the patient had suffered from a one-hit injury or from second-impact syndrome.
Factors that Contributed to Patient Injury
The two most common factors contributing to neonatal patient injuries were selection and management of therapy (39 percent) and patient assessment issues (37 percent). Selection and management of therapy refers to clinical decisions related to delivery: vaginal, operative vaginal, and cesarean section.
Patient assessment issues contributed to patient injury when important information was not considered. An example in neonatal claims is failure to estimate and document fetal weight prior to proceeding with a vaginal delivery. Shoulder dystocia with brachial plexus injuries prompted reviews of these types of decisions. Decisions that did not include an estimate of neonatal weight were viewed as having inadequate patient assessments.
In children older than neonates, issues involving patient assessment were the most common factor contributing to patient harm (36 to 42 percent of the claims in each age group). In these cases, inadequate assessments were often identified by physician experts in cases with incorrect diagnoses. Important information was not collected or was not factored into the diagnosis.
The most common patient assessment issue was failure to appreciate and reconcile relevant signs, symptoms, and test results. In these cases, clinicians failed to recognize the clinical picture from the available information, including patient history, reported symptoms, physical exam, and test results.

Other examples of inadequate assessments included failure or delay in ordering diagnostic tests, inadequate history and physical (including allergies), misinterpretation of diagnostic studies, and over reliance on negative findings in test results on patients with continued symptoms.
Contributing factors for neonate age group (<1 month):
| Number of claims | Percent | |
|---|---|---|
| Selection and management of therapy | 174 | 39% |
| Patient assessment issues | 164 | 37% |
| Communication among providers | 98 | 22% |
| Technical performance | 86 | 19% |
| Insufficient/lack of documentation | 74 | 17% |
| Patient factors | 67 | 15% |
| Communication between patient/family and providers | 65 | 15% |
Contributing factors for first-year age group (1 to 11 months):
| Number of claims | Percent | |
|---|---|---|
| Patient assessment issues | 41 | 42% |
| Insufficient/lack of documentation | 20 | 21% |
| Communication between patient/family and providers | 16 | 16% |
| Selection and management of therapy | 16 | 16% |
| Communication among providers | 16 | 16% |
| Failure/delay in obtaining consult/referral | 16 | 16% |
| Patient factors | 15 | 15% |
Contributing factors for child age group (1 to 9 years):
| Number of claims | Percent | |
|---|---|---|
| Patient assessment issues | 115 | 39% |
| Communication between patient/family and providers | 64 | 22% |
| Patient factors | 63 | 21% |
| Technical performance | 51 | 17% |
| Selection and management of therapy | 50 | 17% |
Contributing factors for teenager age group (10 to 17 years):
| Number of claims | Percent | |
|---|---|---|
| Patient assessment issues | 138 | 36% |
| Patient factors | 94 | 25% |
| Communication between patient/family and providers | 74 | 19% |
| Technical performance | 63 | 17% |
| Communication among providers | 58 | 15% |
| Insufficient/lack of documentation | 58 | 15% |
A healthy female newborn was seen for well-baby visits at two, four, six, and nine months. She received the appropriate vaccines. At the one-year visit, three vaccines were given. The baby had received the first three pneumococcal vaccines on previous visits and was due for the last one.
For an unknown reason, the infant did not receive the fourth pneumococcal vaccine. It was not clear from the documentation if the fourth vaccine was not available due to manufacturer supply problems or if the mother had refused because the baby had already received three vaccines during that office visit. No waiver of vaccination was signed by the mother.
One month later, the baby was evaluated for a rash on her face. The fourth pneumococcal vaccine was not given.
Three months later, the physician’s office sent a form to the daycare with a notice that the baby had not received all of her required vaccinations. The mother later testified that she did not receive a letter and had not been notified by the daycare center.
At 18 months of age, the patient had another well-baby office visit, receiving all the required vaccinations except the fourth pneumococcal vaccine. No documentation indicated the reason.
Two weeks later, the baby became ill and was taken to the emergency department. She was diagnosed with fulminant pneumococcal meningitis. She expired two days later.
In the claim filed by the parents, their expert stated that the standard of care requires physicians to have a system in place to notify them and parents when vaccines are overdue. He opined that the physician missed opportunities to give the fourth pneumococcal vaccine, and, if it had been given, the patient would not have contracted meningitis.
Defense experts stated that the vaccine could have been given at the regular 15-month visit, but the mother did not take the baby to the office then. She testified she was told that the baby did not need a visit at 15 months. The defendant also stated that if the vaccine had been given at the 18-month visit, there would not have been adequate time for immunity to build before she contracted the illness.
The communication breakdown contributed to the death of an infant. The system failure points to the importance of processes that support physicians in providing ongoing care to infants.
A three-year-old boy presented to the emergency department with a four-day history of coughing and swelling of his neck. His mother took him to the emergency department, where he was diagnosed with a pneumomediastinum from a tracheal tear.
A surgeon performed a bronchoscopy, and the patient was intubated. It was determined that the tear would heal on its own with the support of the endotracheal tube. The tear was healing well with minimal edema.
An intensivist provided care to the heavily sedated patient, who developed airway secretions due to an upper respiratory infection. He noted in the record that the patient had a repeat bronchoscopy that showed ongoing respiratory secretions and secretion-related bronchospasms.
After several days, the patient’s condition was improving, so the intensivist planned a trial extubation for the next day. After the extubation, the patient would be placed on continuous positive airway pressure (CPAP). All equipment needed for reintubation was confirmed to be in the patient’s room.
During the night, nurses noted a large amount of thick white sputum. The patient failed two spontaneous breathing trials. This information was documented, but the intensivist was unaware of the results. The intensivist later reported that the patient had a successful trial prior to extubation but this observation was not documented. The patient was extubated and placed on CPAP and high-flow nasal cannula.
An hour later, the patient was noted to have difficulty breathing and stridor. Although his oxygen saturation was decreasing, it improved to some degree each time he was suctioned. A respiratory therapist called the intensivist, who ordered bilevel positive airway pressure.
A short time later, the patient went into respiratory failure, and manual ventilation was initiated. The patient had no pulse, so compressions were started. Atropine was not available for about 45 minutes. The intensivist decided to reintubate the patient due to drops in blood pressure (86/44 mm Hg) and oxygen saturation (87 percent) and an increasing heart rate (110 bpm). Intubation was successful but complicated by increased secretions. After secretions were addressed, the patient’s color returned to normal and heart rate and oxygen saturation improved.
The patient was later diagnosed with hypoxic injury resulting in quadriplegia and severe cognitive and speech impairment. He needs 24-hour care.
Expert opinions were mixed. Some experts said that, considering the two failed spontaneous breathing trials, the extubation should have been performed in an operating room. The night nurses and intensivist should have communicated in preparation for the extubation. Experts also believed that a pediatric anesthesiologist should have been consulted prior to extubation to monitor the patient’s condition following extubation and to assist with any needed reintubation. They criticized the inadequate documentation and questioned why the patient had such a severe outcome with such a short resuscitation time.
Study Discussion
The types of problems experienced by pediatric patients change as they grow older. Neonates and infants in their first year of life were more vulnerable than older children. In this claims analysis, children less than one year of age experienced high-severity injuries at almost twice the rate of children older than one year.
Neonates may experience complications due to difficult labor and delivery. They also face congenital conditions that may not be readily diagnosed and treated.
Children older than one year experienced more injuries from trauma, communicable disease, and malignancies. Teenagers experienced trauma and illness, and teenaged females may also face the dangers of pregnancy and childbirth.
This wide spectrum of development added to the challenges of diagnosing and treating pediatric patients. Clinicians need the assistance of reliable systems, such as those that prompt vaccinations at appropriate intervals and track test results for ill children.
Communication breakdowns between patients/families and providers occurred in 15 to 22 percent of pediatric patient claims, depending on the age group. Inadequate communication resulted in incomplete information to make an accurate diagnosis and in failure to adhere to discharge instructions. Communication failures also resulted in inadequate guidance for parents on conditions that required immediate care, thus limiting a physician’s ability to treat a patient in a timely manner.
A critical time frame for communication follows pediatric surgery. Physicians and their staff members should be attuned to concerns communicated by parents. Staff members need to know when to notify the physician about a parent’s call. The calls provide the first opportunity to address life-threatening conditions, such as obstructed airways, serious allergic reactions, and spreading infections.
In every age group, physician reviewers identified cases with inadequate assessments. Important information may be missed if the physician does not conduct a thorough history and physical exam.
System failures accounted for a significant number of patient injuries. Failing to track orders for diagnostic tests resulted in lost test results. Failing to call critical test results or diagnostic findings to treating physicians delayed treatments.
Early recognition of a patient’s changing status is essential when providing interventions. It requires effective monitoring and documentation, communication among treating physicians, rapid response team implementation, and thorough patient assessments.
This study also highlights the importance of good documentation. The quality of the medical record can be a significant factor in defending a claim that is filed years later.
Adhering to these strategies improves the physician’s ability to provide high-quality care and to successfully defend care.
Risk Mitigation Strategies
The following strategies can assist physicians in preventing some of the concerns identified in this study:
 For Neonates
For Neonates
- Become familiar with the National Institute of Child Health and Human Development (NICHD) nomenclature and participate with nurses in regular fetal monitoring learning activities. The ability to identify fetal heart rate (FHR) patterns predictive of metabolic acidemia is essential to collaborate on clinical interventions effectively.
- Obtain electronic fetal monitoring certification from one of the certifying bodies available for physicians, and regularly update fetal monitoring interpretation skills. Require certification as part of the credentialing process.
- Engage in dialogue about the FHR tracing and assign a category and care plan that both the physician and nurse can agree on.
- Implement an early warning system that outlines vital sign parameters and requires immediate bedside evaluation and escalation of care when necessary.
- Respond without delay when a nurse requests a physician assessment.
- Develop an effective chain-of-command policy that can be activated when conflicts about diagnosis and treatment cannot be resolved.
- Conduct drills to ensure 30-minute response times for emergency cesarean section deliveries.
- Carry out simulations of low-frequency/high-severity obstetric emergencies so staff members are prepared for infrequent events, such as obstetric hemorrhage, shoulder dystocia, eclamptic seizures, sepsis, umbilical cord prolapse, amniotic fluid embolism, and neonatal resuscitation.
- Hold education programs for the entire staff with up-to-date information about safety and technical skills of operative vaginal delivery.
- Estimate and document fetal weight when considering vacuum-assisted vaginal delivery. Plan the exit strategy, such as calling the cesarean section team in advance in case the extraction is unsuccessful.
- Implement a protocol for the care of newborns after vacuum delivery to monitor for scalp swelling consistent with caput, subgaleal hematoma, or cephalohematoma.
 For Children Ages One Month to 17 Years
For Children Ages One Month to 17 Years
- Ensure quality documentation. Documentation is essential for coordinating quality care and defending a claim that may not be filed until years after the alleged injury. In this study, 3 percent of pediatric claims were filed more than 10 years after care was provided.
- Conduct careful reevaluations when patients return with the same or worsening symptoms. If no new information comes to light, consider a second opinion or referral to a specialist. In this study, the most common allegation for children older than one month was failure, delay, or wrong diagnosis. Inadequate patient assessments most commonly contributed to patient injury.
- Ensure an adequate exchange of information. Communication with younger pediatric patients can be very challenging, and the problem is compounded when English is a second language for parents. Utilize translation services if communication is difficult.
- Provide parents with information to help them recognize when a sick child requires emergency care. Train office staff to recognize the types of concerns raised by parents during phone calls that should prompt immediate assessment and treatment.
- Engage the patient/parents to ensure accurate histories and assist in the diagnostic process. Take time to explore patient complaints, especially when a patient returns to the office with continued or worsening symptoms. Diagnosis and treatment depend on skilled patient assessments. Even though patients/parents may be unreliable historians, complaints are the first opportunity to gather information.
- Train office staff to be attuned to calls and concerns voiced by the parents of patients who have recently had surgery. Infections can be difficult to diagnose, especially following surgery. Physicians are often contacted when patients are unable to determine whether symptoms are a normal part of recovery or complications that need medical assistance. A call may be the first opportunity to intervene in a life-threatening condition.
- Document clinical exams and histories clearly.
- Document the details—including any follow-up instructions—when telephone advice is given by physicians or clinical staff.
- Develop a clear policy on tracking diagnostic tests and referrals. Patients do not always follow instructions or diagnostic test orders. The tracking process alerts staff and physicians when test results or referrals have not been received, possibly saving patients’ lives and protecting physicians from malpractice claims.
- Evaluate parents’ understanding of the treatment plan, follow-up care, or medication plan. Nonadherence may not always be willful resistance. Often, parents don’t understand discharge instructions, or they fail to receive adequate instructions. Consider using the teach-back or show-back method. Provide written instructions in a language the parents can read.
- Ask parents about their intentions to follow instructions or purchase medications. An inability to pay for medications or follow-up appointments may impede care and treatment. Asking questions creates opportunities to understand the parents’ level of understanding and any concerns about affordability. If parents admit they have a limited ability to pay for medications or follow-up appointments, provide a list of community services to help the patient receive needed treatment.
A patient safety risk manager is always available to provide industry-leading expertise. For more information, call (800) 421-2368 or contact us by email.
The guidelines suggested here are not rules, do not constitute legal advice, and do not ensure a successful outcome. The ultimate decision regarding the appropriateness of any treatment must be made by each healthcare provider considering the circumstances of the individual situation and in accordance with the laws of the jurisdiction in which the care is rendered.
J11800 03/19