Hospitalist Closed Claims Study
The Doctors Company conducted a review of hospital medicine claims that closed between 2015 and 2018. This study was based on claims and lawsuits filed against almost 1,900 hospitalists insured by The Doctors Company. There were 238 hospitalist claims.
During COVID-19, the Time Is Right to Evaluate Risks Faced by Hospitalists
“If we hadn’t started the hospitalist field 24 years ago, we would have had to invent it now,” says Robert M. Wachter, MD, a professor and chair of the Department of Medicine at the University of California, San Francisco, and the person who coined the term “hospitalist” in 1996. Hospitalists have become leaders, not just within their departments, but within their institutions, based on expertise in caring for critically ill patients. This leadership role has been solidified—and complicated—by COVID-19.
Now, we can expect that people who have delayed seeing providers will arrive at their physician’s office or the emergency department with more advanced disease than if they had accessed healthcare six months ago—thus possibly landing in the care of a hospitalist.1
Such treatment delays for assorted non-COVID-19 conditions may lead to a demographic shift in hospitalists’ patients: Patients could be, on average, younger than usual. This could change how patient complaints present, increasing diagnostic difficulties and risks to patients.
Add to this that hospitalists are also facing communication challenges intensified by layers of PPE, and all the other challenges presented by the pandemic—including our evolving understanding of the disease itself. For instance, hospitalists are finding out in real time how to treat COVID-19 patients whose blood clotting proteins place them at elevated risk of harm from deep vein thrombosis or pulmonary embolism.2
Therefore, the time is right to identify what has led to claims against hospitalists in the past and to elevate awareness of problematic system and cognitive factors that can contribute to adverse events and subsequent suits.
“Hospitalists have become leaders in patient safety and system improvement,” says Dr. Wachter, in part because the specialty coalesced around the idea that hospitalists could both take care of patients and, as specialists in caring for the very sick, see how to make hospitals better.
And in so doing, hospitalists can mitigate their risk of claims.
References
- Gandhi TK, Singh H. Reducing the risk of diagnostic error in the COVID-19 era. J. Hosp. Med. 2020 June;15(6):363-366. Published Online May 18, 2020. Accessed September 11, 2020. https://www.journalofhospitalmedicine.com/jhospmed/article/222266/hospital-medicine/reducing-risk-diagnostic-error-covid-19-era
- MGH News and Public Affairs. COVID-19 and blood clots. Harvard Medical School. Published September 9, 2020. Accessed September 15, 2020. https://hms.harvard.edu/news/covid-19-blood-clots
Regardless of the outcome, all hospitalist claims against our members that closed within this time frame were included in this analysis. This approach helps us better understand what motivates patients to pursue claims and helps us gain a broader overview of the system failures and processes that result in patient harm.
This study includes expert insights and brief summaries of illustrative cases and focuses on the following areas:
- Most common patient injuries.
- Most common types of hospitalist malpractice claims.
- Injury severity.
- Factors contributing to patient injury.
- Strategies for mitigating risk.
This analysis of hospitalist malpractice claims began by studying patients’ injuries to understand the full scope of harm. Physician experts for both the plaintiffs/patients and the defendants/physicians reviewed claims and conducted medical record reviews. Our clinical analysts drew from these sources to gain an accurate and unbiased understanding of actual patient injuries.
Based on our review, we categorized each case based on several attributes. These clinical drivers helped us to focus on the causes of patient harm and the things that prompted patients or their families to file claims and suits.
We identified factors that led to patients’ injuries, and physician reviewers evaluated each claim to determine whether the standard of care was met. Contributing factor categories included clinical judgment, technical skill, patient behaviors, communication, clinical systems, clinical environments, and documentation.
Our team studies all aspects of the claim and identifies risk mitigation strategies that physicians can use to decrease the risk of injury, thereby improving the quality of care.
Patient Injuries
Hospitalists’ patients suffered a variety of injuries. The 10 most common injuries that prompted claims or suits included:
Patients may suffer more than one harm, so the total is greater than 100 percent.
Injury Severity
High-severity injuries occur in a higher percentage of hospitalists’ claims than many other specialties. Seventy-two percent of hospitalists’ patients who filed claims experienced a high-severity injury. This has remained consistent since 2007.
Hospitalist Patient Injury Severity (2015-2018)
Hospitalist Patient Injury Severity (2007-2014)
In contrast, high-severity patient injuries in internal medicine made up 59 percent of their claims. More internal medicine injuries were medium severity (32 percent) compared with 20 percent medium severity for hospitalists’ patients.
Internal Medicine Patient Injury Severity (2015-2018)
Indemnity and Expense
Thirty-two percent of hospital medicine claims resulted in a payment to the patient or their family.
$452,674
Mean indemnity paid in
hospital medicine claims
$159,193
Mean expense paid in
hospital medicine claims
Similarly, general internal medicine physicians’ claims resulted in payments in 32 percent of those claims.
$279,240
Mean indemnity paid in
internal medicine claims
$118,236
Mean expense paid in
internal medicine claims
$250,000
Median indemnity paid for
hospital medicine claims
$109,242
Median expense paid for
hospital medicine claims
$175,000
Median indemnity paid for
internal medicine claims
$87,748
Median expense paid for
internal medicine claims
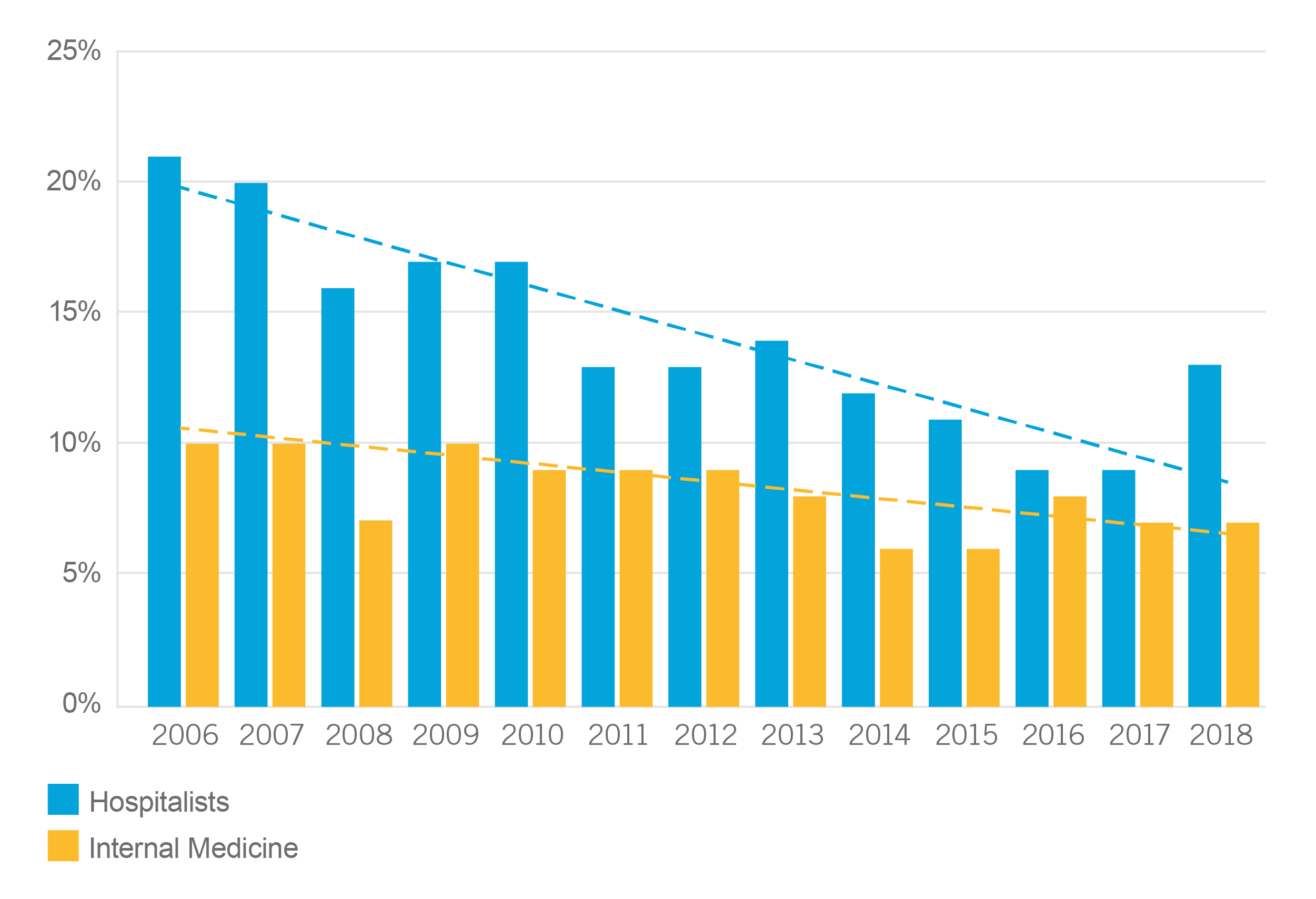
Rate of Claims per 100 Full-Time Equivalents
The rate of claims for hospitalists has declined almost every year from 2006 (21 percent) until 2017 (9 percent). The rate of claims jumped in 2018 to 13 percent.
Internal medicine claims have declined following a similar pattern, but the rate for internal medicine peaked in 2008 at 11 percent and declined to 7 percent in 2017 and 2018.
Types of Claims
There were three primary types of hospital medicine claims.
These case types make up 90 percent of hospitalist claims.
Diagnosis-Related Claims
In diagnosis-related claims, the most common diagnoses were:
The factors that contributed to patient injury in diagnosis-related claims for pulmonary embolism included failure to order diagnostic tests; failure to establish a differential diagnosis; failure to appreciate and reconcile relevant signs, symptoms, and test results; insufficient documentation of clinical rationale; and premature discharge.
A 56-year-old male with a history of hypertension and reflux presented to the emergency department (ED) complaining of right upper quadrant pain. An x-ray showed right lower lobe infiltrates. The patient’s oxygen saturation was 95 percent. His vital signs were within normal limits and he had no lower leg swelling or calf pain.
The patient was admitted with the diagnosis of community-acquired pneumonia. He was started on antibiotics.
The following day, the patient’s oxygen saturation was 85 percent. He was started on three liters of oxygen. His arterial blood gasses were low, he had scant hemoptysis and was febrile. He received a respiratory treatment and was started on Lovenox 40 mg and Lasix. A chest CT scan was negative for pulmonary emboli. The impression was hypoxia secondary to infiltrates and bacteremia.
The patient’s oxygen saturation was 96 percent. An echocardiogram was negative for right-sided failure.
On day three, the patient was evaluated by a physician assistant. The patient stated that he was feeling better, experienced no shortness of breath, and was ambulating. He was afebrile and his lungs were clear. However, his sputum had gram-positive cocci.
The fourth day of his admission to the hospital, the patient was again evaluated by the physician assistant. She noted that the patient was no longer on oxygen, but his saturation levels remained at 95 percent. The patient’s chest x-ray showed improvement. The patient was advised not to fly for one week.
On day five, the patient was discharged and again advised not to fly for a week.
On day eight, the patient flew home. When he arrived, he complained of dizziness, chest pain, and shortness of breath. He went to the ED, where he arrested. Resuscitation attempts were unsuccessful.
The cause of death was determined to be a massive new saddle pulmonary embolism. When questioned, the wife stated that the patient had been cleared to fly.
Expert opinions were mixed upon review. Plaintiff’s experts stated that the chest CT with angiography should have been repeated. Defense experts were supportive of the care, stating that the symptoms of fever, shortness of breath, and chest pain were consistent with pneumonia and pulmonary emboli, but the CT was negative for pulmonary emboli. Also, the patient’s sputum grew staphylococci, which was consistent with pneumonia. The patient improved on antibiotics and steroids. The patient received Lovenox but refused TED hose. They felt that the workup and diagnosis were reasonable. The patient had not complied with discharge instructions. The case was dismissed.
This case is about alleged failure to diagnose and treat pulmonary embolism, resulting in the patient’s death.
The patient was a 69-year-old obese male with a history of smoking, hypertension, cardiomyopathy, GERD, elevated lipids, atrial fibrillation, and obstructive sleep apnea. He presented to the ED complaining of shortness of breath, dizziness, and chest pain on the left side, but no radiating pain. He had been experiencing these symptoms for three days.
Lab tests showed critically low potassium and magnesium. The patient was started on an IV fluids with potassium and magnesium added. The patient’s heart rate was 103 BPM and irregular. An EKG showed atrial fibrillation. The patient was admitted to the hospital.
The hospitalist noted that the patient’s shortness of breath was becoming progressively worse. The patient complained of dizziness and pain in his thigh and shoulder. The hospitalist ordered a CT coronary angiogram and D-dimer. Initially the CT and D-dimer were ordered stat, but then ordered in addition to the routine ED studies. For some reason, the CT was not performed.
The shift ended and the hospitalist went home. The D-dimer was not performed because blood collected in the ED was not adequate for this added test. Since the D-dimer was not ordered stat, it was scheduled for 7:00 AM. The hospitalist did not check on the status of the test before leaving the hospital.
The second hospitalist assumed care at 8:00 PM. The departing hospitalist did not discuss the condition of this critically ill patient during the handoff. The patient appeared to be stable.
At 4:00 AM, a nurse called the hospitalist because of the patient’s elevated respiratory rate. Within 30 minutes, the patient arrested. Another physician responded but was unable to resuscitate the patient. An autopsy confirmed the presence of pulmonary emboli.
Plaintiff’s and defense experts were not supportive of the care provided. They criticized the ED physician for not ordering a pulmonary CT scan and diagnosing pulmonary embolism. Although the hospitalist did have pulmonary embolism included under differential diagnosis, experts believed that it was not given a high enough priority, considering that signs and symptoms were consistent with pulmonary embolism. After a history of three days of shortness of breath, leg swelling, chest pain, and atrial fibrillation, the order for lab tests should have been stat. The laboratory should have notified the hospitalist and nurses if they were unable to do the test in addition to the other studies ordered in the ED.
Experts also criticized the quality of the handoff from the first to the second hospitalist regarding this critically ill patient. The first hospitalist did not tell the second hospitalist about the pending D-dimer study.
Experts were mixed in their judgment regarding whether the patient would have experienced a different outcome if clinicians had been more aggressive in diagnosing the patient. Some felt that an earlier diagnosis would have enabled administration of unfractionated heparin, and the patient would have survived. The jury decided in favor of the plaintiffs.
This case alleged delay in diagnosis of spinal epidural abscess that resulted in incomplete quadriplegia. The patient was a 49-year-old male with a history of smoking, IV drug abuse, hepatitis C, cirrhosis, hypertension, and chronic pain.
On day one, the patient presented to an outpatient clinic with complaints of headache, neck pain, and sore throat. After the initial assessment, the patient was discharged with instructions to go to an ED if his symptoms became worse.
Three days later, the patient presented to the ED complaining of headache. A CT of the patient’s head was within normal limits. He was given pain medication and discharged.
Ten days later, the patient went to an urgent care center complaining of headache and neck pain that radiated down his back and arms. The patient was sent to the ED, where a lumbar puncture was performed. The spinal fluid had 650 WBCs with 80 percent neutrophils, but no bacteria. Blood cultures were drawn.
The patient was diagnosed with viral meningitis, treated, and discharged. Spinal epidural abscess was included in the differential diagnosis, but the ED physician did not order an MRI.
The next day, blood cultures were reported as positive for staphylococcus. The patient was called at home and admitted to the hospital with a diagnosis of staph meningitis and placed on antibiotics. His neurological functions were intact, but the patient continued to complain of headache and photophobia.
The second day of admission, the patient complained of severe neck pain. Even with morphine, the patient was writhing in pain. When called by the nurse, a second hospitalist ordered Dilaudid but did not evaluate the patient.
The third day of hospitalization, a foley catheter was placed for urinary retention. The nurse documented pain in the patient’s neck and legs but did not notify a physician. That evening, a nurse contacted the hospitalist to report that the patient could not move his legs. The hospitalist discontinued the patient’s morphine, instructed the nurse to monitor the patient’s condition but did not go to the patient’s room to evaluate his condition. The night nurse noted the same neurological symptoms but did not notify the hospitalist.
Early the following morning, an attending physician was told about the patient’s condition. He evaluated the patient and called for a stat MRI, which showed cord compression. The patient was immediately transferred to another hospital for surgery.
Surgery was too late. The patient suffered incomplete quadriplegia.
Experts were critical of the care received by the patient. Plaintiffs stated that the ED physician misinterpreted the lumbar puncture, stating that the findings were not consistent with meningitis. He should have ordered an MRI to rule out spinal epidural abscess and should have admitted the patient on antibiotics.
The first hospitalist should have evaluated the patient himself and ordered a CT when the patient experienced urinary retention. The second hospitalist was criticized for failing to evaluate the patient when notified by nurses.
The nurses were criticized for not communicating the urgency of the patient’s symptoms and demanding a physician evaluation when the patient began to exhibit neurological symptoms. When they received no response, they should have followed the chain of command policy to seek help for the patient.
Some defense experts were supportive of some aspects of the care, stating that the patient had an atypical presentation. Other defense experts were not supportive. They stated that the ED physician should have admitted the patient and ordered an MRI, because the patient exhibited classic signs of SEA. They opined that neurological changes should have prompted the first hospitalist to assess the patient and order consultations from infectious disease and neurology. He should have ordered an MRI with gadolinium when the patient developed urinary retention.
This case settled for a large sum.
Spinal epidural abscess was the second-most common missed or delayed diagnosis. Factors that contributed to patient injury in diagnosis-related claims for spinal epidural abscess included delays in ordering diagnostic tests, communication among providers regarding the patient’s condition, and failure to appreciate and reconcile relevant signs, symptoms, and test results. In these cases, symptoms warranted studies to rule out spinal epidural abscess but were not ordered. In some cases, nurses were aware of a patient’s changing neurological status but failed to notify the attending physician. In other cases, the attending physician was aware but failed to take definitive steps to diagnose the problem and timely refer the patient for surgical intervention.
Improper Management of Treatment Claims
The second-most common driver of claims was improper management of treatment (28 percent). In these management cases, physician reviewers found deficiencies with:
There were 19 other deficiencies found, which each were represented in 17 percent or fewer claims.
The most common diagnoses associated with improper management of treatment included:
Diagnoses that were each found in 3 percent of claims studied included cardiac arrest, congestive heart failure, cerebral artery occlusion with infarction, pneumonia, vascular insufficiency to intestine, nontraumatic hemoperitoneum, and respiratory arrest.
The factors identified by physician reviewers as contributing to patient harm for pulmonary embolism included inadequate patient assessments and selection and management of therapy. In one case, the hospitalist was alleged to have failed to order an insertion of an inferior vena cava filter. However, it was determined that the patient was too fragile to endure the procedure. In another case, the patient experienced an intracranial bleed. When a DVT was suspected, a doppler study was ordered, but the patient could not be placed on anticoagulants. The patient expired before the test could be performed. Both cases were dismissed.
In the cases of sepsis, there were questions about timely diagnosis and appropriateness of treatment. Physician reviewers noted failure to appreciate and reconcile relevant signs, symptoms, and test results, thus delaying interventions. In some of these cases, patients did not follow treatment plans.
In the acute myocardial infarction cases, it was noted that initial diagnoses were incorrect because the physicians failed to develop a differential diagnosis. In some cases, there was a delay in ordering diagnostic tests that would have facilitated a correct diagnosis.
A 77-year-old patient was admitted to the hospital for dehydration and bedsores. She had a history of chronic urinary tract infections. The patient was dependent for all activities of daily living.
The hospitalist who admitted the patient ordered medical management and physical therapy. Nurses documented that the patient refused to eat her meals, to get out of bed, or to comply with treatment.
Eventually, the patient’s wounds healed, but nurses continued to chart the patient’s refusal to eat, to get out of bed, or to do physical therapy.
Late on the second day of admission, the patient appeared to be confused and lethargic. The hospitalist ordered a urinalysis with cultures and CBC. The patient’s urine was cloudy, and her WBC was 17.3 with a left shift. The hospitalist ordered a stat chest x-ray and charted early sepsis. The chest x-ray was negative. No medications were ordered.
The next day, the patient was placed in a wheelchair. She refused care and was lethargic. Her blood pressure was 107/68, her temperature was 97, and her oxygen saturation was 91 percent.
The staff left the patient and returned two hours later. They found the patient without a pulse or respiration. The patient had a “do not resuscitate” order, so no measures were taken to resuscitate the patient. The patient’s death was determined to be caused by sepsis.
The patient’s family filed a claim alleging negligent care. They stated that the patient had been left in the wheelchair for too long without supervision by staff. They challenged the hospitalist’s care by stating that he should have ordered antibiotics based on the elevated WBC and left shift. The patient’s confusion and lethargy, with her history of chronic urinary tract infections, should have prompted administration of IV antibiotics. Appropriate care could have prevented urosepsis and death.
Defense experts were supportive, stating that the patient’s vital signs did not suggest sepsis. Also, they pointed out that the elevated WBC could have been due to a nonspecific infection. They agreed with the hospitalist’s decision to order a stat chest x-ray and to wait for the reading before ordering additional medications. Defense experts also pointed to the patient’s healed bedsores as evidence of good care. The case settled.
Improper Medication Management Claims
The third driver of hospitalist claims was improper medication management. The factors that contributed to patient injury included:
Patient assessment issues included inadequate history and physicals and failure to appreciate and reconcile relevant signs, symptoms, and test results. Physician reviewers also cited failure or delay in ordering diagnostic tests.
Another factor in improper medication management was selection and management of therapy. This most often was related to failure to order medications or ordering medications that were contraindicated by other medications.
The third factor that impacted medication management was communication among providers regarding the patient’s condition. Communication failures were sometimes due to the failure to review the medical record or to inadequate handoffs. Important information was not communicated during transitions in care.
A 79-year-old male presented to the ED with complaints of pain in his left arm and head after falling at home the previous evening. He had a history of dysphagia, GERD, osteoporosis, rheumatoid arthritis, COPD, hypertension, anemia, DVT, and spinal surgeries. He used oxycodone for chronic pain.
A CT of the patient’s head was negative. X-rays of his arm showed a fracture of the right humerus. The patient’s hemoglobin was 9.2 and his blood pressure was 88/55. Oxygen saturation was 96 percent on two liters of oxygen. The patient was started on IV fluids.
The patient was admitted by the hospitalist, who ordered subcutaneous heparin every eight hours, CBCs every 48 hours, coagulation studies every 24 hours, and morphine as needed for pain. The patient was transferred to a medical/surgical floor with no telemetry ordered.
An orthopedic surgeon was consulted. He recommended conservative treatment with possible surgery after medical assessments were complete. The patient was placed in a sling and treated with pain medication.
Later that afternoon, nurses noted tachycardia with a blood pressure of 73/51. The patient’s pulse was 119. The hospitalist ordered a bolus of fluids, which increased his blood pressure to 87/55.
An hour later, the rapid response team was called because the patient’s blood pressure had dropped, oxygen saturation was 85 percent, and the patient vomited coffee ground emesis. The responding physician ordered Narcan, expecting the cause to be narcotics.
Monitored vital signs showed blood pressures 80–90/55–65. Hemoglobin was reported as 5.6, so the hospitalist discontinued heparin. He ordered more laboratory tests for iron.
The hospitalist conducted a history and physical. His differential diagnosis included GI bleeding. He ordered a GI consultation, noting that the patient’s hemoglobin had dropped significantly in eight hours. The hospitalist documented that the patient was transferred to the intensive care unit (ICU), but the order to transfer the patient was never written.
Nurses called the hospitalist to report patient complaints of pain and repeat vomiting that still showed coffee ground emesis. The hospitalist ordered morphine, a nasogastric tube, IV fluids, Zofran, vitamin K, and a transfer to the ICU.
Before the patient could be transferred, he became unresponsive. He was resuscitated following a respiratory arrest and transferred to the ICU. A chest x-ray showed worsening infiltrates in the base of the right lung, which was thought to be due to aspiration. The following morning’s chest x-ray showed extensive bilateral infiltrates. The patient was diagnosed with a GI bleed, anemia, leukopenia, thrombocytopenia, and coagulopathy. The following day, the patient expired.
Some plaintiff's and defense experts were not supportive of the assessments and care received by the patient. They criticized the hospitalist for the delayed history and physical, and for not transferring the patient to the ICU. The hospitalist failed to document signs and symptoms of bleeding and inappropriately ordered narcotic pain medications. Despite the patient’s vomiting, the patient’s history of dysphagia did not prompt precautions to prevent aspiration. The GI consult was delayed.
Other defense experts had mixed reviews of the care. They opined that the patient should have been admitted to the ICU due to the likely GI bleeding and aspiration. They criticized the delay in ordering a GI consultation. Their view was that the patient’s problem was not a narcotic overload. The case settled as a result of the critical opinions of the hospitalist’s care.
Causes of Patient Harm
Patient harm comes from a variety of causes. In some cases, physicians failed to follow protocols. In other cases, the patient’s presentation was not typical and did not point to a specific diagnosis. There were examples of chronic conditions that were assumed to be the cause of current symptoms rather than the manifestation of a new disease entity.
The largest number of cases revealed weaknesses in systems and processes that were depended upon by nurses and physicians. Information can be difficult to locate in some electronic health records (EHRs) or obscured by lengthy progress notes resulting from copying and pasting over-documentation. On occasion, tests were not performed, or test results were not delivered, or reports were not received by treating physicians.
Communication between nurses and hospitalists sometimes failed. Handoffs between hospitals did not convey critical information, and efforts to reach physicians in other specialties were sometimes unsuccessful.
Top 10 Risk Mitigation Strategies for Hospitalists
The following strategies may help hospitalists avoid some of the issues uncovered by this study:
- Ensure effective handoff procedures during hospitalization and at discharge.
- Communicate with everyone involved in the patient’s care, including patient, family, prior-treating physician, and patient care team members.
- Introduce yourself and your role.
- Sit down and talk to the patient using their name and eye contact.
- Document your plan and rationale, including any changes in plan.
- Be sure to document patient noncompliance.
- Use quotes for patient comments related to noncompliance.
- Evaluate the need for physical examination when notified of a change in an inpatient’s condition.
- If in doubt, go see the patient for a bedside evaluation.
- Be mindful of what you tell nursing staff on the phone, as they will chart your exact comment with quotation marks.
- Always consider a differential diagnosis early in treatment.
- Follow up on all laboratory tests and procedure reports.
- Review test and lab results that were not available prior to patient discharge.
- Ensure notification of primary care physician and patient of abnormal results after discharge.
- Do not delay consultations or testing.
- Be careful relying on curbside consultation and always consider asking the specialist to examine and evaluate the patient.
- Ask for a second opinion.
- Advanced practice practitioners should consult supervising physician if needed.
- Documentation is your silent witness: Document clearly and completely in the patient medical record.
- Know the approved abbreviation list for the facility, as they are not all the same.
- Review the medical record thoroughly. Understand facility EHR protocols and where to find information in the EHR.
- If the patient was seen in the ER previously for related symptoms, review the ER record.
- Ask for help from nursing staff if you cannot find something in the medical record.
Conclusion
In many ways, hospitalists provide essential functions in healthcare as the medical profession has specialized and subspecialized. Hospitalists provide coordination of care for hospitalized patients.
Providing care to large numbers of acutely ill patients exposes hospitalists to claims and lawsuits, some of which are primarily directed at other clinicians. There are things that hospitalists can do to reduce the chances of patients being harmed and hospitalists being named in claims or lawsuits.
Hospitalists provide the essential link between patients and specialists, and among a variety of clinicians. Teamwork requires effective working relationships, attention to important test results, communication of important information during handoffs, and comprehensive documentation.
The guidelines suggested here are not rules, do not constitute legal advice, and do not ensure a successful outcome. The ultimate decision regarding the appropriateness of any treatment must be made by each healthcare provider considering the circumstances of the individual situation and in accordance with the laws of the jurisdiction in which the care is rendered.
09/20